{"title":"全身血浆免疫球蛋白 G 水平不足的适应性回归,作为治疗暴发性溃疡性结肠炎的紧急结肠切除术后的康复生物标记物。","authors":"Alexander T Hawkins, Jun W Um, Amosy E M'Koma","doi":"10.1177/1179552217746692","DOIUrl":null,"url":null,"abstract":"<p><p>Restorative proctocolectomy (RPC) with ileal pouch-anal anastomosis (IPAA) is the standard surgical treatment for ulcerative colitis (UC). Emergency colectomies are performed for fulminant colitis (ie, toxic megacolon, profuse bleeding, perforation, or sepsis). The RPC and IPAA involve manipulation of the proximal ileum, which may influence the essential physiological function of gut-associated lymphoid tissues. Circulating plasma immunoglobulin G (p-IgG) deficiency is observed in patients with fulminant UC. In addition, increased levels have been reported in colonic tissues of active UC compared with quiescent disease. We aimed to examine levels of p-IgG for clinical evaluation following emergency colectomies in patients with fulminant UC compared with patients with quiescent disease having elective RPC operations. In total 45 patients received an ileoanal pouch (IAP) due to UC. In all, 27 patients were men and 18 were women. The mean age was 34 years (range: 18-55). Because of fulminant UC, 26 patients had emergency subtotal colectomies with terminal ileostomy (TI). During second operation, the rectum was excised, and an IAP with diverting loop ileostomy (DLI) was performed. Nineteen patients had elective operations and had colectomies performed in conjunction with the pouch operation. Mucosectomy was performed in all groups. As a last procedure, the DLI was closed. Blood samples for immunoglobulin G (IgG) analyses were collected from each patient before the colectomy, after the colectomy with TI (before construction of the pouch), during the period with pouches (prior to DLI closure), and at 1, 2, and 3 years and at mean 13.7 years (range: 10-20) after DLI closure. Immunoglobulin G was determined by immunonephelometric assay technique. The statistics were analyzed by analysis of variance and linear regression. Preoperatively, p-IgG was significantly lower in the patients who had emergency operations compared with the group that had elective operations, 9.9 ± 3.0 vs 11.5 ± 3.3 g/L (<i>P</i> < .03). During the manipulative period with TI and/or DLI, the p-IgG levels were increased in both points, but the increase was not statistically significant (<i>P</i> = .26 and <i>P</i> = .19). During functional IAP at 1, 2, and 3 years and at mean 13.7 years (range: 10-20), there was a statistical increase in p-IgG levels (<i>P</i> < .002, <i>P</i> < .005, <i>P</i> < .005, and <i>P</i> < .0001) compared with preoperative levels. These changes did not correlate with episodes of pouchitis (<i>P</i> = .51). In patients having elective operations, p-IgG did not change preoperatively. After 12 months with functional pouches, the p-IgG levels were similar in both groups to the elective patient group preoperatively. In conclusion, p-IgG was found to be significantly lower in the emergency surgery patients compared with the elective surgery group preoperatively. This difference was probably due to increased losses and impaired gut lymphoid tissue production of IgG in the acute fulminant phase of UC. After 12 months of DLI closure, significant differences were no longer found between the emergency and elective surgery groups. Restoration and increased p-IgG levels after RPC would be due to an exaggerated response to make up for lower precolectomy values and may be interpreted as a rehabilitation biomarker.</p>","PeriodicalId":10382,"journal":{"name":"Clinical Medicine Insights. Gastroenterology","volume":"10 ","pages":"1179552217746692"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/bb/10.1177_1179552217746692.PMC5734426.pdf","citationCount":"0","resultStr":"{\"title\":\"Adaptive Returns of Deficient Systemic Plasma Immunoglobulin G Levels as Rehabilitation Biomarker After Emergency Colectomy for Fulminant Ulcerative Colitis.\",\"authors\":\"Alexander T Hawkins, Jun W Um, Amosy E M'Koma\",\"doi\":\"10.1177/1179552217746692\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Restorative proctocolectomy (RPC) with ileal pouch-anal anastomosis (IPAA) is the standard surgical treatment for ulcerative colitis (UC). Emergency colectomies are performed for fulminant colitis (ie, toxic megacolon, profuse bleeding, perforation, or sepsis). The RPC and IPAA involve manipulation of the proximal ileum, which may influence the essential physiological function of gut-associated lymphoid tissues. Circulating plasma immunoglobulin G (p-IgG) deficiency is observed in patients with fulminant UC. In addition, increased levels have been reported in colonic tissues of active UC compared with quiescent disease. We aimed to examine levels of p-IgG for clinical evaluation following emergency colectomies in patients with fulminant UC compared with patients with quiescent disease having elective RPC operations. In total 45 patients received an ileoanal pouch (IAP) due to UC. In all, 27 patients were men and 18 were women. The mean age was 34 years (range: 18-55). Because of fulminant UC, 26 patients had emergency subtotal colectomies with terminal ileostomy (TI). During second operation, the rectum was excised, and an IAP with diverting loop ileostomy (DLI) was performed. Nineteen patients had elective operations and had colectomies performed in conjunction with the pouch operation. Mucosectomy was performed in all groups. As a last procedure, the DLI was closed. Blood samples for immunoglobulin G (IgG) analyses were collected from each patient before the colectomy, after the colectomy with TI (before construction of the pouch), during the period with pouches (prior to DLI closure), and at 1, 2, and 3 years and at mean 13.7 years (range: 10-20) after DLI closure. Immunoglobulin G was determined by immunonephelometric assay technique. The statistics were analyzed by analysis of variance and linear regression. Preoperatively, p-IgG was significantly lower in the patients who had emergency operations compared with the group that had elective operations, 9.9 ± 3.0 vs 11.5 ± 3.3 g/L (<i>P</i> < .03). During the manipulative period with TI and/or DLI, the p-IgG levels were increased in both points, but the increase was not statistically significant (<i>P</i> = .26 and <i>P</i> = .19). During functional IAP at 1, 2, and 3 years and at mean 13.7 years (range: 10-20), there was a statistical increase in p-IgG levels (<i>P</i> < .002, <i>P</i> < .005, <i>P</i> < .005, and <i>P</i> < .0001) compared with preoperative levels. These changes did not correlate with episodes of pouchitis (<i>P</i> = .51). In patients having elective operations, p-IgG did not change preoperatively. After 12 months with functional pouches, the p-IgG levels were similar in both groups to the elective patient group preoperatively. In conclusion, p-IgG was found to be significantly lower in the emergency surgery patients compared with the elective surgery group preoperatively. This difference was probably due to increased losses and impaired gut lymphoid tissue production of IgG in the acute fulminant phase of UC. After 12 months of DLI closure, significant differences were no longer found between the emergency and elective surgery groups. Restoration and increased p-IgG levels after RPC would be due to an exaggerated response to make up for lower precolectomy values and may be interpreted as a rehabilitation biomarker.</p>\",\"PeriodicalId\":10382,\"journal\":{\"name\":\"Clinical Medicine Insights. Gastroenterology\",\"volume\":\"10 \",\"pages\":\"1179552217746692\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-12-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/bb/10.1177_1179552217746692.PMC5734426.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179552217746692\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179552217746692","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Adaptive Returns of Deficient Systemic Plasma Immunoglobulin G Levels as Rehabilitation Biomarker After Emergency Colectomy for Fulminant Ulcerative Colitis.
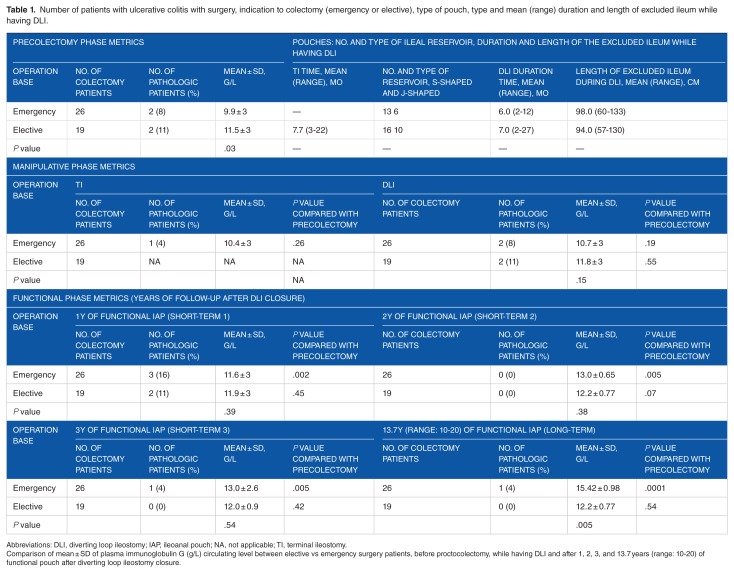
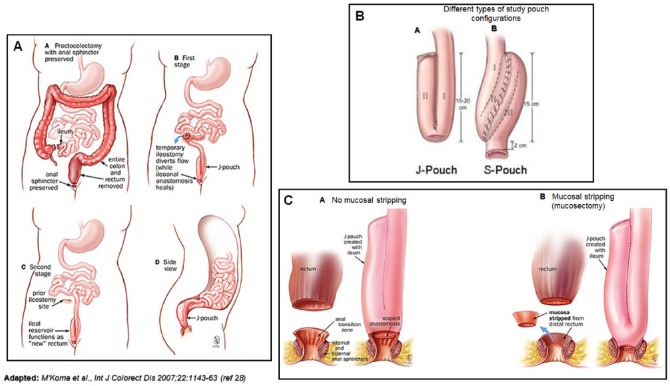
Restorative proctocolectomy (RPC) with ileal pouch-anal anastomosis (IPAA) is the standard surgical treatment for ulcerative colitis (UC). Emergency colectomies are performed for fulminant colitis (ie, toxic megacolon, profuse bleeding, perforation, or sepsis). The RPC and IPAA involve manipulation of the proximal ileum, which may influence the essential physiological function of gut-associated lymphoid tissues. Circulating plasma immunoglobulin G (p-IgG) deficiency is observed in patients with fulminant UC. In addition, increased levels have been reported in colonic tissues of active UC compared with quiescent disease. We aimed to examine levels of p-IgG for clinical evaluation following emergency colectomies in patients with fulminant UC compared with patients with quiescent disease having elective RPC operations. In total 45 patients received an ileoanal pouch (IAP) due to UC. In all, 27 patients were men and 18 were women. The mean age was 34 years (range: 18-55). Because of fulminant UC, 26 patients had emergency subtotal colectomies with terminal ileostomy (TI). During second operation, the rectum was excised, and an IAP with diverting loop ileostomy (DLI) was performed. Nineteen patients had elective operations and had colectomies performed in conjunction with the pouch operation. Mucosectomy was performed in all groups. As a last procedure, the DLI was closed. Blood samples for immunoglobulin G (IgG) analyses were collected from each patient before the colectomy, after the colectomy with TI (before construction of the pouch), during the period with pouches (prior to DLI closure), and at 1, 2, and 3 years and at mean 13.7 years (range: 10-20) after DLI closure. Immunoglobulin G was determined by immunonephelometric assay technique. The statistics were analyzed by analysis of variance and linear regression. Preoperatively, p-IgG was significantly lower in the patients who had emergency operations compared with the group that had elective operations, 9.9 ± 3.0 vs 11.5 ± 3.3 g/L (P < .03). During the manipulative period with TI and/or DLI, the p-IgG levels were increased in both points, but the increase was not statistically significant (P = .26 and P = .19). During functional IAP at 1, 2, and 3 years and at mean 13.7 years (range: 10-20), there was a statistical increase in p-IgG levels (P < .002, P < .005, P < .005, and P < .0001) compared with preoperative levels. These changes did not correlate with episodes of pouchitis (P = .51). In patients having elective operations, p-IgG did not change preoperatively. After 12 months with functional pouches, the p-IgG levels were similar in both groups to the elective patient group preoperatively. In conclusion, p-IgG was found to be significantly lower in the emergency surgery patients compared with the elective surgery group preoperatively. This difference was probably due to increased losses and impaired gut lymphoid tissue production of IgG in the acute fulminant phase of UC. After 12 months of DLI closure, significant differences were no longer found between the emergency and elective surgery groups. Restoration and increased p-IgG levels after RPC would be due to an exaggerated response to make up for lower precolectomy values and may be interpreted as a rehabilitation biomarker.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


