{"title":"急性髓性白血病合并心内血栓表现为急性肢体缺血。","authors":"Rajiv Bharat Kharwar, Kamal Sharma, Sharad Jain","doi":"10.4250/jcu.2016.24.2.174","DOIUrl":null,"url":null,"abstract":"A 50-year-old female presented to our emergency department with complaints of acute onset pain in left lower limb for last 5 days. Her previous history was unremarkable. Physical examination revealed a pulse rate of 90 per minute, blood pressure of 120/76 mm Hg and normal jugular venous pulse. The left lower limb was cold and pale. Her left femoral, left popliteal, left dorsalis pedis and left posterior tibial arterial pulsations were absent. All other arterial pulsations were normally present. Cardiac and respiratory examinations were within normal limits. Electrocardiogram was within normal limits with normal sinus rhythm. A diagnosis of acute limb ischemia was made and an emergency computed tomographic angiography of infra renal aorta with both the lower limbs was done. There was a partial filling defect of the aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery with distal reformation by collateral from the arteries of the contralateral limb (Fig. 1). Two dimensional echocardiography showed a large (2.0 × 3.0 cm) mobile thrombus at the apico-septal region of the left ventricle along with normal ejection fraction of 60% (Fig. 2A, Supplementary movie 1). The three dimensional (3D) nature of the thrombus was better appreciated on transthoracic 3D echocardiography (Fig. 2B, Supplementary movie 2). Hematologic studies revealed anemia, with hemoglobin level of 10 g/dL, thrombocytopenia (30 platelets/nL) and leucocytocis (240 white blood cells/nL). Peripheral smear showed 95% blast cells which were peroxidase negative (Fig. 3). Bone marrow aspiration confirmed the diagnosis of acute myeloid leukemia (French American British type M2). Aortic with left ileo-femoral thromboembolectomy was done to salvage the limb. Intra venous heparin therapy was started for left ventricular thrombus. Patient was transferred to the oncology department where induction phase of chemotherapy was started according to acute myeloid leukemia management protocol. \n \n \n \nFig. 1 \n \nComputed tomographic angiography of aorta with both lower limb. There is a partially occluding thrombus at the lower aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery from the origin. A: The left ... \n \n \n \n \n \nFig. 2 \n \nTransthoracic echocardiography. A: Two dimensional echocardiography in apical four chamber view (A) showing normal sized LV with a 2.0 × 3.0 cm thrombus at the apico-septal region. B: The three dimensional (3D) structure of the thrombus is better ... \n \n \n \n \n \nFig. 3 \n \nPeripheral blood smear at 400 × magnification (A) and 1000 × magnification (B) using Wright stain. A: There are plenty of blast in the peripheral smear which can be identified by hyperchromatic nuclei with a raised nucleus/cytoplasm ratio. ... \n \n \n \nPatients with acute leukemia are at an increased risk of both thrombosis as well as bleeding. Severe haemorrhagic complications are seen in acute promyelocytic leukemiausually secondary to disseminated intravascular coagulation. Thrombotic complications are rarely reported. There are very few reports of acute limb ischemia due to large artery occlusion in acute myeloid leukemia.1) None of the previously reported cases had left ventricular thrombus. To our knowledge, this is the first report of acute myeloid leukemia having left ventricular thrombus and left lower limb thromboembolism on presentation. \n \nThe pathology of coagulopathy in acute leukemia is complex. It is determined by an interplay between various procoagulant factors (like tissue factor, cancer procoagulant factor, prothrombotic cytokines) and anticoagulant and fibrinolytic factors released or expressed by the leukemic cells.2) \n \nDue to scarcity of occurrence of thrombotic complications in acute myeloid leukemia, no large scale studies are available for guiding management of this complication. Thrombolytic and anticoagulation therapy is not without risk as patient are also at increased risk of bleeding due to simultaneous occurrence of thrombocytopenia and disseminated intravascular coagulation. Prompt diagnosis of underlying leukemia and initiation of appropriate anti leukemia treatment are keys to reducing overall morbidity and mortality.","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 2","pages":"174-6"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.2.174","citationCount":"4","resultStr":"{\"title\":\"Acute Myeloid Leukemia with Intracardiac Thrombus Presenting as Acute Limb Ischemia.\",\"authors\":\"Rajiv Bharat Kharwar, Kamal Sharma, Sharad Jain\",\"doi\":\"10.4250/jcu.2016.24.2.174\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 50-year-old female presented to our emergency department with complaints of acute onset pain in left lower limb for last 5 days. Her previous history was unremarkable. Physical examination revealed a pulse rate of 90 per minute, blood pressure of 120/76 mm Hg and normal jugular venous pulse. The left lower limb was cold and pale. Her left femoral, left popliteal, left dorsalis pedis and left posterior tibial arterial pulsations were absent. All other arterial pulsations were normally present. Cardiac and respiratory examinations were within normal limits. Electrocardiogram was within normal limits with normal sinus rhythm. A diagnosis of acute limb ischemia was made and an emergency computed tomographic angiography of infra renal aorta with both the lower limbs was done. There was a partial filling defect of the aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery with distal reformation by collateral from the arteries of the contralateral limb (Fig. 1). Two dimensional echocardiography showed a large (2.0 × 3.0 cm) mobile thrombus at the apico-septal region of the left ventricle along with normal ejection fraction of 60% (Fig. 2A, Supplementary movie 1). The three dimensional (3D) nature of the thrombus was better appreciated on transthoracic 3D echocardiography (Fig. 2B, Supplementary movie 2). Hematologic studies revealed anemia, with hemoglobin level of 10 g/dL, thrombocytopenia (30 platelets/nL) and leucocytocis (240 white blood cells/nL). Peripheral smear showed 95% blast cells which were peroxidase negative (Fig. 3). Bone marrow aspiration confirmed the diagnosis of acute myeloid leukemia (French American British type M2). Aortic with left ileo-femoral thromboembolectomy was done to salvage the limb. Intra venous heparin therapy was started for left ventricular thrombus. Patient was transferred to the oncology department where induction phase of chemotherapy was started according to acute myeloid leukemia management protocol. \\n \\n \\n \\nFig. 1 \\n \\nComputed tomographic angiography of aorta with both lower limb. There is a partially occluding thrombus at the lower aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery from the origin. A: The left ... \\n \\n \\n \\n \\n \\nFig. 2 \\n \\nTransthoracic echocardiography. A: Two dimensional echocardiography in apical four chamber view (A) showing normal sized LV with a 2.0 × 3.0 cm thrombus at the apico-septal region. B: The three dimensional (3D) structure of the thrombus is better ... \\n \\n \\n \\n \\n \\nFig. 3 \\n \\nPeripheral blood smear at 400 × magnification (A) and 1000 × magnification (B) using Wright stain. A: There are plenty of blast in the peripheral smear which can be identified by hyperchromatic nuclei with a raised nucleus/cytoplasm ratio. ... \\n \\n \\n \\nPatients with acute leukemia are at an increased risk of both thrombosis as well as bleeding. Severe haemorrhagic complications are seen in acute promyelocytic leukemiausually secondary to disseminated intravascular coagulation. Thrombotic complications are rarely reported. There are very few reports of acute limb ischemia due to large artery occlusion in acute myeloid leukemia.1) None of the previously reported cases had left ventricular thrombus. To our knowledge, this is the first report of acute myeloid leukemia having left ventricular thrombus and left lower limb thromboembolism on presentation. \\n \\nThe pathology of coagulopathy in acute leukemia is complex. It is determined by an interplay between various procoagulant factors (like tissue factor, cancer procoagulant factor, prothrombotic cytokines) and anticoagulant and fibrinolytic factors released or expressed by the leukemic cells.2) \\n \\nDue to scarcity of occurrence of thrombotic complications in acute myeloid leukemia, no large scale studies are available for guiding management of this complication. Thrombolytic and anticoagulation therapy is not without risk as patient are also at increased risk of bleeding due to simultaneous occurrence of thrombocytopenia and disseminated intravascular coagulation. Prompt diagnosis of underlying leukemia and initiation of appropriate anti leukemia treatment are keys to reducing overall morbidity and mortality.\",\"PeriodicalId\":88913,\"journal\":{\"name\":\"Journal of cardiovascular ultrasound\",\"volume\":\"24 2\",\"pages\":\"174-6\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4250/jcu.2016.24.2.174\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cardiovascular ultrasound\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4250/jcu.2016.24.2.174\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/6/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.2.174","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Acute Myeloid Leukemia with Intracardiac Thrombus Presenting as Acute Limb Ischemia.
A 50-year-old female presented to our emergency department with complaints of acute onset pain in left lower limb for last 5 days. Her previous history was unremarkable. Physical examination revealed a pulse rate of 90 per minute, blood pressure of 120/76 mm Hg and normal jugular venous pulse. The left lower limb was cold and pale. Her left femoral, left popliteal, left dorsalis pedis and left posterior tibial arterial pulsations were absent. All other arterial pulsations were normally present. Cardiac and respiratory examinations were within normal limits. Electrocardiogram was within normal limits with normal sinus rhythm. A diagnosis of acute limb ischemia was made and an emergency computed tomographic angiography of infra renal aorta with both the lower limbs was done. There was a partial filling defect of the aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery with distal reformation by collateral from the arteries of the contralateral limb (Fig. 1). Two dimensional echocardiography showed a large (2.0 × 3.0 cm) mobile thrombus at the apico-septal region of the left ventricle along with normal ejection fraction of 60% (Fig. 2A, Supplementary movie 1). The three dimensional (3D) nature of the thrombus was better appreciated on transthoracic 3D echocardiography (Fig. 2B, Supplementary movie 2). Hematologic studies revealed anemia, with hemoglobin level of 10 g/dL, thrombocytopenia (30 platelets/nL) and leucocytocis (240 white blood cells/nL). Peripheral smear showed 95% blast cells which were peroxidase negative (Fig. 3). Bone marrow aspiration confirmed the diagnosis of acute myeloid leukemia (French American British type M2). Aortic with left ileo-femoral thromboembolectomy was done to salvage the limb. Intra venous heparin therapy was started for left ventricular thrombus. Patient was transferred to the oncology department where induction phase of chemotherapy was started according to acute myeloid leukemia management protocol.
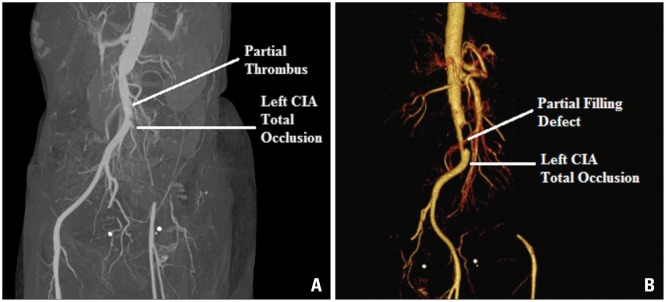
Fig. 1
Computed tomographic angiography of aorta with both lower limb. There is a partially occluding thrombus at the lower aorta just before the bifurcation along with complete thrombotic occlusion of the left common iliac artery from the origin. A: The left ...
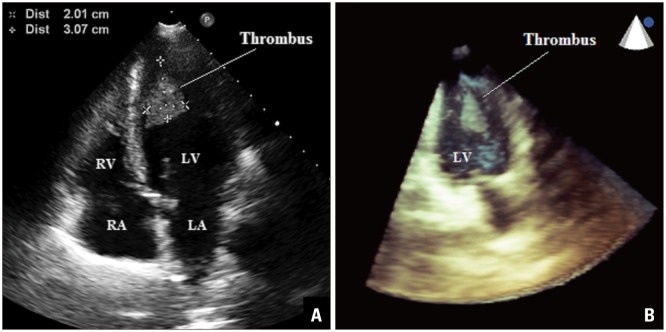
Fig. 2
Transthoracic echocardiography. A: Two dimensional echocardiography in apical four chamber view (A) showing normal sized LV with a 2.0 × 3.0 cm thrombus at the apico-septal region. B: The three dimensional (3D) structure of the thrombus is better ...
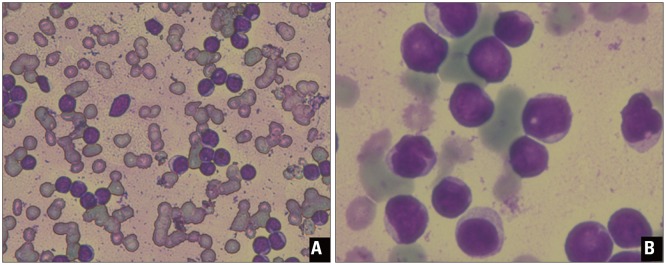
Fig. 3
Peripheral blood smear at 400 × magnification (A) and 1000 × magnification (B) using Wright stain. A: There are plenty of blast in the peripheral smear which can be identified by hyperchromatic nuclei with a raised nucleus/cytoplasm ratio. ...
Patients with acute leukemia are at an increased risk of both thrombosis as well as bleeding. Severe haemorrhagic complications are seen in acute promyelocytic leukemiausually secondary to disseminated intravascular coagulation. Thrombotic complications are rarely reported. There are very few reports of acute limb ischemia due to large artery occlusion in acute myeloid leukemia.1) None of the previously reported cases had left ventricular thrombus. To our knowledge, this is the first report of acute myeloid leukemia having left ventricular thrombus and left lower limb thromboembolism on presentation.
The pathology of coagulopathy in acute leukemia is complex. It is determined by an interplay between various procoagulant factors (like tissue factor, cancer procoagulant factor, prothrombotic cytokines) and anticoagulant and fibrinolytic factors released or expressed by the leukemic cells.2)
Due to scarcity of occurrence of thrombotic complications in acute myeloid leukemia, no large scale studies are available for guiding management of this complication. Thrombolytic and anticoagulation therapy is not without risk as patient are also at increased risk of bleeding due to simultaneous occurrence of thrombocytopenia and disseminated intravascular coagulation. Prompt diagnosis of underlying leukemia and initiation of appropriate anti leukemia treatment are keys to reducing overall morbidity and mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


