Elena Tonkopi, Eline Jahre Wikan, Tor Olav Hovland, Sivert Høgset, Thomas Alexander Kofod, Selasi K Sefenu, Emily Hughes-Ryan, Dakota D Entremont-O Connell, Catherine Gunn, Tanja Holter, Safora Johansen
{"title":"挪威和加拿大的头部、胸部、腹部和骨盆计算机断层扫描诊断参考水平的调查。","authors":"Elena Tonkopi, Eline Jahre Wikan, Tor Olav Hovland, Sivert Høgset, Thomas Alexander Kofod, Selasi K Sefenu, Emily Hughes-Ryan, Dakota D Entremont-O Connell, Catherine Gunn, Tanja Holter, Safora Johansen","doi":"10.1177/20584601221131477","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Computed tomography (CT) contributes to 60% of the collective dose in medical imaging. Literature has demonstrated that patient dose varies across regions and countries. Establishing diagnostic reference levels (DRLs) contributes to the optimization of clinical practices and radiation protection.</p><p><strong>Purpose: </strong>To survey the dose indices (CTDIvol and dose-length product) for frequently performed CT examinations from the chosen hospitals in Norway and Canada and to determine local DRLs (LDRLs) based on the collected data.</p><p><strong>Material and methods: </strong>The survey included eight scanners from two Norwegian hospitals and four scanners from four Canadian hospitals. Dosimetry data were collected for the following routine CT examinations: head, contrast-enhanced thorax, and abdomen and pelvis. Overall 480 adult average-sized patients from Norway and 360 from Canada were included in the survey. The LDRLs were determined as the 75th percentile of distributions of median values of dose indicators from different CT scanners. The differences in dose between scanners were determined using single-factor ANOVA.</p><p><strong>Results: </strong>The LDRLs determined in Norway were higher overall than in Canada. The obtained values were compared to the national DRLs. The dose from several scanners in Norway exceeded national Norwegian DRLs, while Canadian LDRLs were below the Canadian reference levels. The differences between the means of the dose distributions from each scanner were statistically significant (<i>p</i> < 0.05) for all examinations with exception of identical scanners located in the same hospital and using the same protocols.</p><p><strong>Conclusion: </strong>Observed dose variations even in the same hospital, or from the same scanner model confirmed the need for CT protocol optimization.</p>","PeriodicalId":72063,"journal":{"name":"Acta radiologica open","volume":"11 10","pages":"20584601221131477"},"PeriodicalIF":1.0000,"publicationDate":"2022-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c7/69/10.1177_20584601221131477.PMC9549116.pdf","citationCount":"0","resultStr":"{\"title\":\"A survey of local diagnostic reference levels for the head, thorax, abdomen and pelvis computed tomography in Norway and Canada.\",\"authors\":\"Elena Tonkopi, Eline Jahre Wikan, Tor Olav Hovland, Sivert Høgset, Thomas Alexander Kofod, Selasi K Sefenu, Emily Hughes-Ryan, Dakota D Entremont-O Connell, Catherine Gunn, Tanja Holter, Safora Johansen\",\"doi\":\"10.1177/20584601221131477\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Computed tomography (CT) contributes to 60% of the collective dose in medical imaging. Literature has demonstrated that patient dose varies across regions and countries. Establishing diagnostic reference levels (DRLs) contributes to the optimization of clinical practices and radiation protection.</p><p><strong>Purpose: </strong>To survey the dose indices (CTDIvol and dose-length product) for frequently performed CT examinations from the chosen hospitals in Norway and Canada and to determine local DRLs (LDRLs) based on the collected data.</p><p><strong>Material and methods: </strong>The survey included eight scanners from two Norwegian hospitals and four scanners from four Canadian hospitals. Dosimetry data were collected for the following routine CT examinations: head, contrast-enhanced thorax, and abdomen and pelvis. Overall 480 adult average-sized patients from Norway and 360 from Canada were included in the survey. The LDRLs were determined as the 75th percentile of distributions of median values of dose indicators from different CT scanners. The differences in dose between scanners were determined using single-factor ANOVA.</p><p><strong>Results: </strong>The LDRLs determined in Norway were higher overall than in Canada. The obtained values were compared to the national DRLs. The dose from several scanners in Norway exceeded national Norwegian DRLs, while Canadian LDRLs were below the Canadian reference levels. The differences between the means of the dose distributions from each scanner were statistically significant (<i>p</i> < 0.05) for all examinations with exception of identical scanners located in the same hospital and using the same protocols.</p><p><strong>Conclusion: </strong>Observed dose variations even in the same hospital, or from the same scanner model confirmed the need for CT protocol optimization.</p>\",\"PeriodicalId\":72063,\"journal\":{\"name\":\"Acta radiologica open\",\"volume\":\"11 10\",\"pages\":\"20584601221131477\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2022-10-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c7/69/10.1177_20584601221131477.PMC9549116.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta radiologica open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20584601221131477\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta radiologica open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20584601221131477","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
A survey of local diagnostic reference levels for the head, thorax, abdomen and pelvis computed tomography in Norway and Canada.
Background: Computed tomography (CT) contributes to 60% of the collective dose in medical imaging. Literature has demonstrated that patient dose varies across regions and countries. Establishing diagnostic reference levels (DRLs) contributes to the optimization of clinical practices and radiation protection.
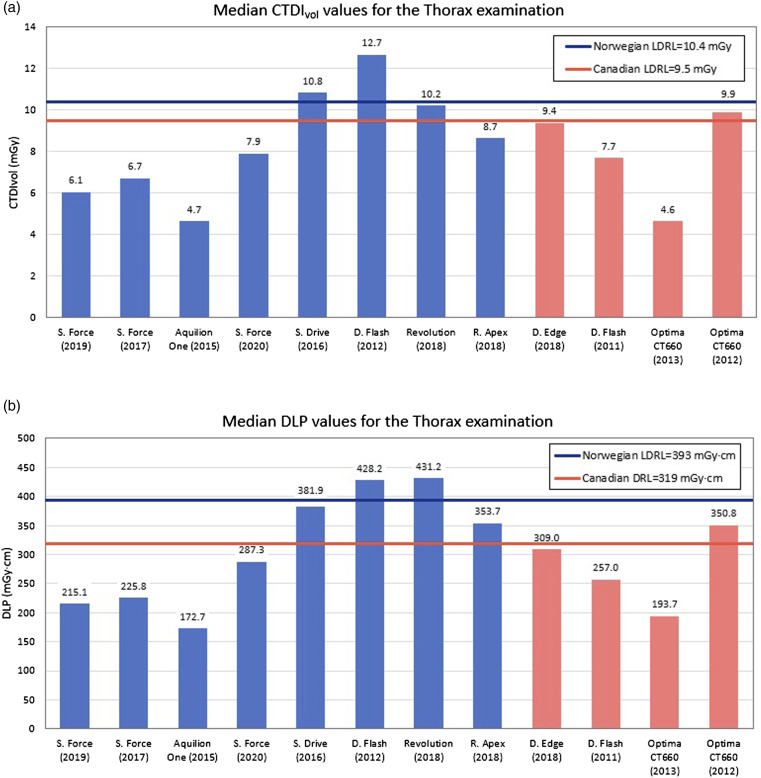
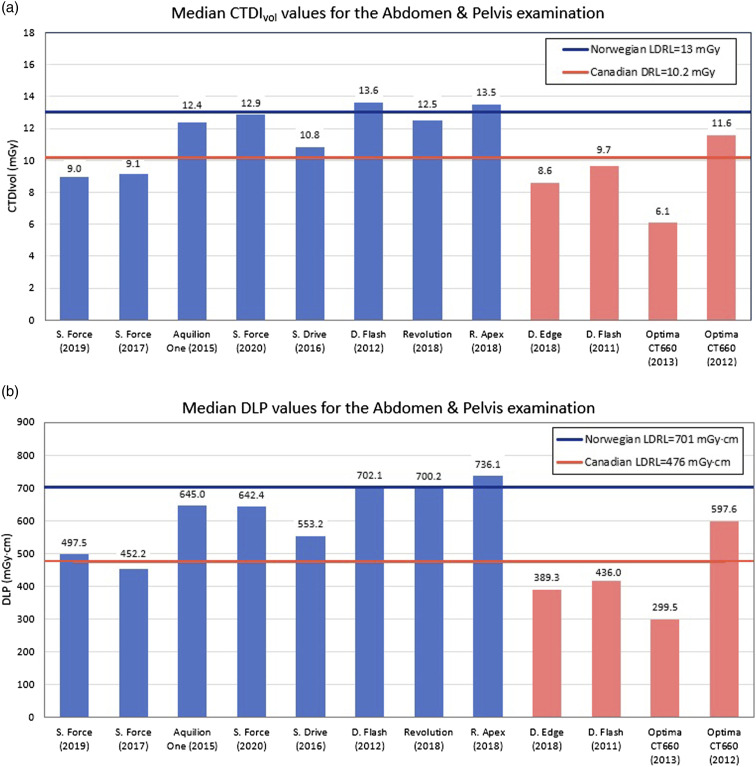
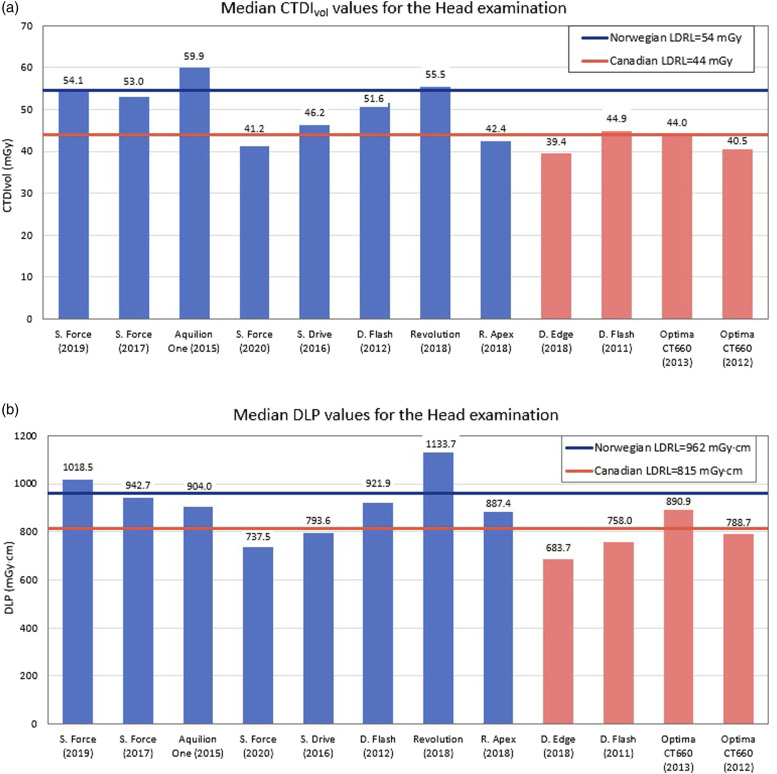
Purpose: To survey the dose indices (CTDIvol and dose-length product) for frequently performed CT examinations from the chosen hospitals in Norway and Canada and to determine local DRLs (LDRLs) based on the collected data.
Material and methods: The survey included eight scanners from two Norwegian hospitals and four scanners from four Canadian hospitals. Dosimetry data were collected for the following routine CT examinations: head, contrast-enhanced thorax, and abdomen and pelvis. Overall 480 adult average-sized patients from Norway and 360 from Canada were included in the survey. The LDRLs were determined as the 75th percentile of distributions of median values of dose indicators from different CT scanners. The differences in dose between scanners were determined using single-factor ANOVA.
Results: The LDRLs determined in Norway were higher overall than in Canada. The obtained values were compared to the national DRLs. The dose from several scanners in Norway exceeded national Norwegian DRLs, while Canadian LDRLs were below the Canadian reference levels. The differences between the means of the dose distributions from each scanner were statistically significant (p < 0.05) for all examinations with exception of identical scanners located in the same hospital and using the same protocols.
Conclusion: Observed dose variations even in the same hospital, or from the same scanner model confirmed the need for CT protocol optimization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


