Ginevra Mills, Bernice Goorah, Shai E Elizur, Weon-Young Son, Michael H Dahan
{"title":"多囊卵巢卵泡分布模式与月经紊乱程度及血清性类固醇水平的关系。","authors":"Ginevra Mills, Bernice Goorah, Shai E Elizur, Weon-Young Son, Michael H Dahan","doi":"10.4274/tjod.galenos.2022.63255","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to examine the associations between follicular distribution pattern (FDP) in polycystic ovaries and menstrual disturbances in women with infertility.</p><p><strong>Materials and methods: </strong>A retrospective review of patients was performed (n=73). Ultrasound images from cycle day 2-5 of a spontaneous or progestin induced menstrual cycle were reviewed. Ovaries were classified as polycystic ovarian morphology (PCOM) if they contained ≥12-follicles measuring 2-9 mm in diameter. Images of PCOM ovaries were classified as having a peripheral cystic pattern (PCP) with follicles arranged at the periphery of the ovary, or general cystic pattern (GCP) if follicles were dispersed heterogeneously throughout the ovarian stroma. Menstrual disturbance was assessed by questionnaire, and oligomenorrhea was defined as cycles >35 days in length.</p><p><strong>Results: </strong>PCP was more strongly associated with menstrual irregularity that GCP. 94% of subjects with bilateral PCP-experienced oligomenorrhea compared with 65% of women with a unilateral PCP ovary [odds ratio (OR) 9; p<0.05]. 29% of women with bilateral GCP ovaries experienced menstrual disturbances, less than bilateral PCP (OR 36; p=0.002), but similar to unilateral PCP (OR 3; p=0.07). Serum testosterone and luteinizing hormone (LH) levels were significantly correlated with the ovarian FDP.</p><p><strong>Conclusion: </strong>There is a relationship between menstrual irregularity or certain types of serum steroids and ovarian morphology. It remains unknown if morphology, testosterone or LH causes the menstrual disturbance or if they are co-initiated by an intervening factor.</p>","PeriodicalId":45340,"journal":{"name":"Turkish Journal of Obstetrics and Gynecology","volume":"19 3","pages":"215-220"},"PeriodicalIF":1.0000,"publicationDate":"2022-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ac/b6/TJOG-19-215.PMC9511927.pdf","citationCount":"0","resultStr":"{\"title\":\"Relationship between the follicular distribution pattern of polycystic ovaries and the degree of menstrual disturbance and serum sex steroid levels.\",\"authors\":\"Ginevra Mills, Bernice Goorah, Shai E Elizur, Weon-Young Son, Michael H Dahan\",\"doi\":\"10.4274/tjod.galenos.2022.63255\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aimed to examine the associations between follicular distribution pattern (FDP) in polycystic ovaries and menstrual disturbances in women with infertility.</p><p><strong>Materials and methods: </strong>A retrospective review of patients was performed (n=73). Ultrasound images from cycle day 2-5 of a spontaneous or progestin induced menstrual cycle were reviewed. Ovaries were classified as polycystic ovarian morphology (PCOM) if they contained ≥12-follicles measuring 2-9 mm in diameter. Images of PCOM ovaries were classified as having a peripheral cystic pattern (PCP) with follicles arranged at the periphery of the ovary, or general cystic pattern (GCP) if follicles were dispersed heterogeneously throughout the ovarian stroma. Menstrual disturbance was assessed by questionnaire, and oligomenorrhea was defined as cycles >35 days in length.</p><p><strong>Results: </strong>PCP was more strongly associated with menstrual irregularity that GCP. 94% of subjects with bilateral PCP-experienced oligomenorrhea compared with 65% of women with a unilateral PCP ovary [odds ratio (OR) 9; p<0.05]. 29% of women with bilateral GCP ovaries experienced menstrual disturbances, less than bilateral PCP (OR 36; p=0.002), but similar to unilateral PCP (OR 3; p=0.07). Serum testosterone and luteinizing hormone (LH) levels were significantly correlated with the ovarian FDP.</p><p><strong>Conclusion: </strong>There is a relationship between menstrual irregularity or certain types of serum steroids and ovarian morphology. It remains unknown if morphology, testosterone or LH causes the menstrual disturbance or if they are co-initiated by an intervening factor.</p>\",\"PeriodicalId\":45340,\"journal\":{\"name\":\"Turkish Journal of Obstetrics and Gynecology\",\"volume\":\"19 3\",\"pages\":\"215-220\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2022-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ac/b6/TJOG-19-215.PMC9511927.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Turkish Journal of Obstetrics and Gynecology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4274/tjod.galenos.2022.63255\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish Journal of Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/tjod.galenos.2022.63255","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Relationship between the follicular distribution pattern of polycystic ovaries and the degree of menstrual disturbance and serum sex steroid levels.
Objective: This study aimed to examine the associations between follicular distribution pattern (FDP) in polycystic ovaries and menstrual disturbances in women with infertility.
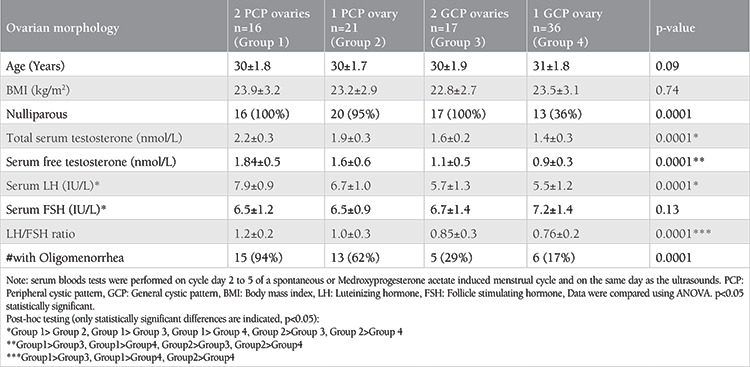
Materials and methods: A retrospective review of patients was performed (n=73). Ultrasound images from cycle day 2-5 of a spontaneous or progestin induced menstrual cycle were reviewed. Ovaries were classified as polycystic ovarian morphology (PCOM) if they contained ≥12-follicles measuring 2-9 mm in diameter. Images of PCOM ovaries were classified as having a peripheral cystic pattern (PCP) with follicles arranged at the periphery of the ovary, or general cystic pattern (GCP) if follicles were dispersed heterogeneously throughout the ovarian stroma. Menstrual disturbance was assessed by questionnaire, and oligomenorrhea was defined as cycles >35 days in length.
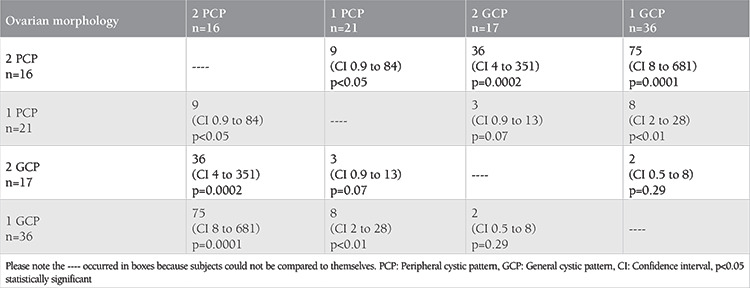
Results: PCP was more strongly associated with menstrual irregularity that GCP. 94% of subjects with bilateral PCP-experienced oligomenorrhea compared with 65% of women with a unilateral PCP ovary [odds ratio (OR) 9; p<0.05]. 29% of women with bilateral GCP ovaries experienced menstrual disturbances, less than bilateral PCP (OR 36; p=0.002), but similar to unilateral PCP (OR 3; p=0.07). Serum testosterone and luteinizing hormone (LH) levels were significantly correlated with the ovarian FDP.
Conclusion: There is a relationship between menstrual irregularity or certain types of serum steroids and ovarian morphology. It remains unknown if morphology, testosterone or LH causes the menstrual disturbance or if they are co-initiated by an intervening factor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


