Cailin Nieuwenhuizen, Tshiphiri Netshidzivhani, Johan Potgieter
{"title":"在南非比勒陀利亚建立血红蛋白A2参考区间:回顾性二级数据分析。","authors":"Cailin Nieuwenhuizen, Tshiphiri Netshidzivhani, Johan Potgieter","doi":"10.4102/ajlm.v11i1.1841","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Haemoglobinopathies are one of the most common inherited diseases worldwide. Quantification of haemoglobin A<sub>2</sub> is necessary for the diagnosis of the beta thalassaemia trait. In this context, it is important to have a reliable reference interval for haemoglobin A<sub>2</sub> and a local reference range for South Africa has not been established.</p><p><strong>Objective: </strong>This study aimed to establish reference intervals for haemoglobin A<sub>2</sub> using stored patient laboratory data.</p><p><strong>Methods: </strong>This descriptive study used retrospective data to evaluate haemoglobin A<sub>2</sub> levels determined using high-performance liquid chromatography at the National Health Laboratory Service haematology laboratory in Pretoria, South Africa. All tests performed from 01 October 2012 to 31 December 2020 were screened for inclusion; of these, 144 patients' data met the selection criteria. The reference interval was calculated using descriptive statistics (mean and standard deviation) with a 95% confidence interval.</p><p><strong>Results: </strong>Analysed data from enrolled patients showed a normal distribution. The mean age of the patients was 40 years (range: 3-84 years). The reference interval for haemoglobin A<sub>2</sub> calculated from this data was 2.3% - 3.6%. The minimum haemoglobin A<sub>2</sub> was 2.3% and the maximum was 3.9% with a mean of 2.95% and a standard deviation of 0.357%.</p><p><strong>Conclusion: </strong>A normal reference interval has been established for the population served by the laboratory that will assist with accurate diagnosis of the beta thalassaemia trait. This reference interval may also be useful to other laboratories that employ the same technology, especially smaller laboratories where obtaining a sufficiently large number of normal controls may be challenging.</p>","PeriodicalId":45412,"journal":{"name":"African Journal of Laboratory Medicine","volume":" ","pages":"1841"},"PeriodicalIF":1.0000,"publicationDate":"2022-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9453124/pdf/","citationCount":"0","resultStr":"{\"title\":\"Establishment of haemoglobin A<sub>2</sub> reference intervals in Pretoria, South Africa: A retrospective secondary data analysis.\",\"authors\":\"Cailin Nieuwenhuizen, Tshiphiri Netshidzivhani, Johan Potgieter\",\"doi\":\"10.4102/ajlm.v11i1.1841\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Haemoglobinopathies are one of the most common inherited diseases worldwide. Quantification of haemoglobin A<sub>2</sub> is necessary for the diagnosis of the beta thalassaemia trait. In this context, it is important to have a reliable reference interval for haemoglobin A<sub>2</sub> and a local reference range for South Africa has not been established.</p><p><strong>Objective: </strong>This study aimed to establish reference intervals for haemoglobin A<sub>2</sub> using stored patient laboratory data.</p><p><strong>Methods: </strong>This descriptive study used retrospective data to evaluate haemoglobin A<sub>2</sub> levels determined using high-performance liquid chromatography at the National Health Laboratory Service haematology laboratory in Pretoria, South Africa. All tests performed from 01 October 2012 to 31 December 2020 were screened for inclusion; of these, 144 patients' data met the selection criteria. The reference interval was calculated using descriptive statistics (mean and standard deviation) with a 95% confidence interval.</p><p><strong>Results: </strong>Analysed data from enrolled patients showed a normal distribution. The mean age of the patients was 40 years (range: 3-84 years). The reference interval for haemoglobin A<sub>2</sub> calculated from this data was 2.3% - 3.6%. The minimum haemoglobin A<sub>2</sub> was 2.3% and the maximum was 3.9% with a mean of 2.95% and a standard deviation of 0.357%.</p><p><strong>Conclusion: </strong>A normal reference interval has been established for the population served by the laboratory that will assist with accurate diagnosis of the beta thalassaemia trait. This reference interval may also be useful to other laboratories that employ the same technology, especially smaller laboratories where obtaining a sufficiently large number of normal controls may be challenging.</p>\",\"PeriodicalId\":45412,\"journal\":{\"name\":\"African Journal of Laboratory Medicine\",\"volume\":\" \",\"pages\":\"1841\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2022-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9453124/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"African Journal of Laboratory Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/ajlm.v11i1.1841\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Laboratory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/ajlm.v11i1.1841","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Establishment of haemoglobin A2 reference intervals in Pretoria, South Africa: A retrospective secondary data analysis.
Background: Haemoglobinopathies are one of the most common inherited diseases worldwide. Quantification of haemoglobin A2 is necessary for the diagnosis of the beta thalassaemia trait. In this context, it is important to have a reliable reference interval for haemoglobin A2 and a local reference range for South Africa has not been established.
Objective: This study aimed to establish reference intervals for haemoglobin A2 using stored patient laboratory data.
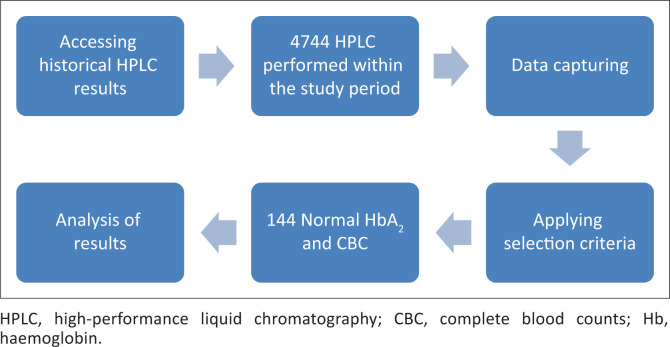
Methods: This descriptive study used retrospective data to evaluate haemoglobin A2 levels determined using high-performance liquid chromatography at the National Health Laboratory Service haematology laboratory in Pretoria, South Africa. All tests performed from 01 October 2012 to 31 December 2020 were screened for inclusion; of these, 144 patients' data met the selection criteria. The reference interval was calculated using descriptive statistics (mean and standard deviation) with a 95% confidence interval.
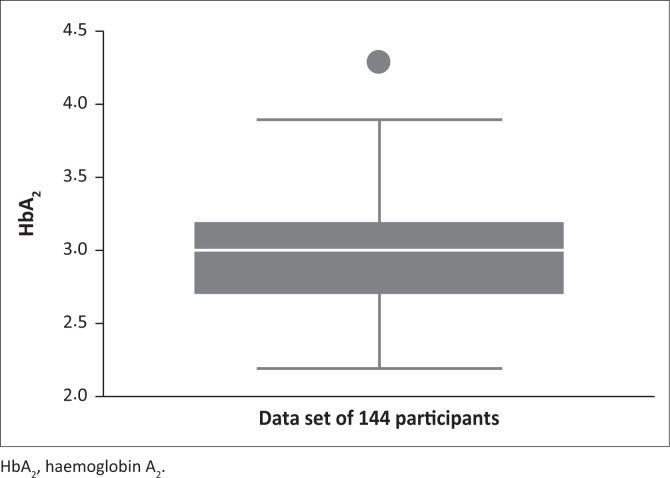
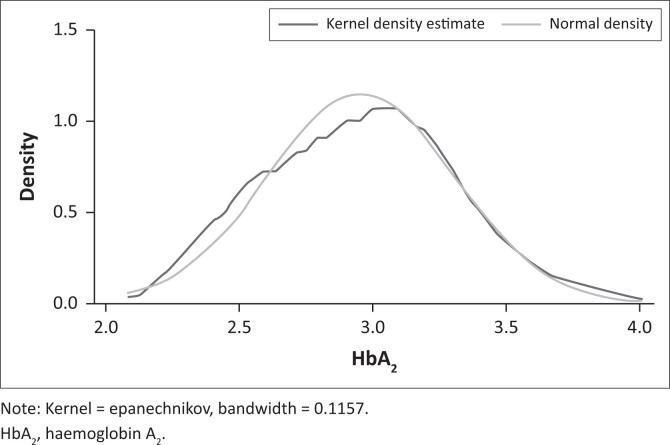
Results: Analysed data from enrolled patients showed a normal distribution. The mean age of the patients was 40 years (range: 3-84 years). The reference interval for haemoglobin A2 calculated from this data was 2.3% - 3.6%. The minimum haemoglobin A2 was 2.3% and the maximum was 3.9% with a mean of 2.95% and a standard deviation of 0.357%.
Conclusion: A normal reference interval has been established for the population served by the laboratory that will assist with accurate diagnosis of the beta thalassaemia trait. This reference interval may also be useful to other laboratories that employ the same technology, especially smaller laboratories where obtaining a sufficiently large number of normal controls may be challenging.
期刊介绍:
The African Journal of Laboratory Medicine, the official journal of ASLM, focuses on the role of the laboratory and its professionals in the clinical and public healthcare sectors,and is specifically based on an African frame of reference. Emphasis is on all aspects that promote and contribute to the laboratory medicine practices of Africa. This includes, amongst others: laboratories, biomedical scientists and clinicians, medical community, public health officials and policy makers, laboratory systems and policies (translation of laboratory knowledge, practices and technologies in clinical care), interfaces of laboratory with medical science, laboratory-based epidemiology, laboratory investigations, evidence-based effectiveness in real world (actual) settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


