Carvallo-Venegas Mauricio, Fuentes-López Elsa Angélica, Andrade-Ortega Antonio de Jesús, Torres-Baranda José Rodrigo, Carrasco-Carrizosa Aldo, Cerrillos-Gutierrez José Ignacio, Andrade-Sierra Jorge
{"title":"肾移植受者感染SARS-CoV-2后播散性组织胞浆菌病、肺结核和巨细胞病毒病","authors":"Carvallo-Venegas Mauricio, Fuentes-López Elsa Angélica, Andrade-Ortega Antonio de Jesús, Torres-Baranda José Rodrigo, Carrasco-Carrizosa Aldo, Cerrillos-Gutierrez José Ignacio, Andrade-Sierra Jorge","doi":"10.1155/2022/8042168","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Infection with SARS-CoV-2 increases the risk of acute graft dysfunction (AGD) in renal transplant recipients (RTR), and the risk of concurrently presenting with opportunistic infections is also increased. There is no current consensus on the management of immunosuppression during SARS-CoV-2 infection in RTR. <i>Case Presentation</i>. A 35-year-old male RTR from a living related donor presented with SARS-CoV-2 infection (January 2021). Two months later, despite alterations to his immunosuppression regimen (tacrolimus (TAC) was reduced by 50%, and the mycophenolic acid (MMF) was suspended with the remission of symptoms), the patient presented with pulmonary tuberculosis, pneumonia due to respiratory syncytial virus (RSV), cytomegalovirus (CMV) pneumonitis, and histoplasmosis (HP). Management was initiated with antituberculosis medications, ganciclovir, antibiotics, and liposomal amphotericin B, and the immunosuppressants were suspended, yet the patient's evolution was catastrophic and the outcome fatal.</p><p><strong>Conclusion: </strong>We recommend that in RTR post-COVID-19, the immunosuppression regimen should be gradually reinstated along with strict vigilance in observing for highly prevalent coinfections (TB, HP, and CMV).</p>","PeriodicalId":30327,"journal":{"name":"Case Reports in Transplantation","volume":" ","pages":"8042168"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9441404/pdf/","citationCount":"1","resultStr":"{\"title\":\"Disseminated Histoplasmosis, Pulmonary Tuberculosis, and Cytomegalovirus Disease in a Renal Transplant Recipient after Infection with SARS-CoV-2.\",\"authors\":\"Carvallo-Venegas Mauricio, Fuentes-López Elsa Angélica, Andrade-Ortega Antonio de Jesús, Torres-Baranda José Rodrigo, Carrasco-Carrizosa Aldo, Cerrillos-Gutierrez José Ignacio, Andrade-Sierra Jorge\",\"doi\":\"10.1155/2022/8042168\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Infection with SARS-CoV-2 increases the risk of acute graft dysfunction (AGD) in renal transplant recipients (RTR), and the risk of concurrently presenting with opportunistic infections is also increased. There is no current consensus on the management of immunosuppression during SARS-CoV-2 infection in RTR. <i>Case Presentation</i>. A 35-year-old male RTR from a living related donor presented with SARS-CoV-2 infection (January 2021). Two months later, despite alterations to his immunosuppression regimen (tacrolimus (TAC) was reduced by 50%, and the mycophenolic acid (MMF) was suspended with the remission of symptoms), the patient presented with pulmonary tuberculosis, pneumonia due to respiratory syncytial virus (RSV), cytomegalovirus (CMV) pneumonitis, and histoplasmosis (HP). Management was initiated with antituberculosis medications, ganciclovir, antibiotics, and liposomal amphotericin B, and the immunosuppressants were suspended, yet the patient's evolution was catastrophic and the outcome fatal.</p><p><strong>Conclusion: </strong>We recommend that in RTR post-COVID-19, the immunosuppression regimen should be gradually reinstated along with strict vigilance in observing for highly prevalent coinfections (TB, HP, and CMV).</p>\",\"PeriodicalId\":30327,\"journal\":{\"name\":\"Case Reports in Transplantation\",\"volume\":\" \",\"pages\":\"8042168\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9441404/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/8042168\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/8042168","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Disseminated Histoplasmosis, Pulmonary Tuberculosis, and Cytomegalovirus Disease in a Renal Transplant Recipient after Infection with SARS-CoV-2.
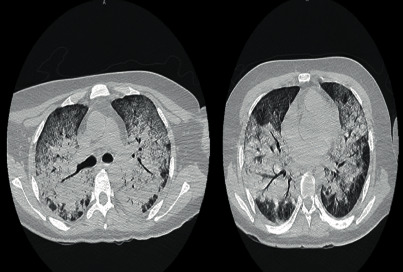
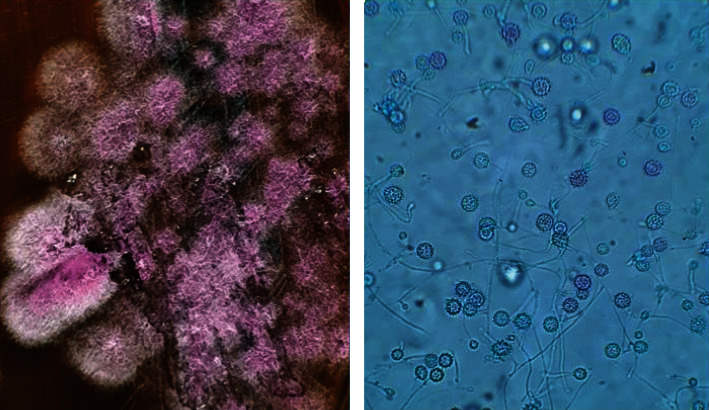
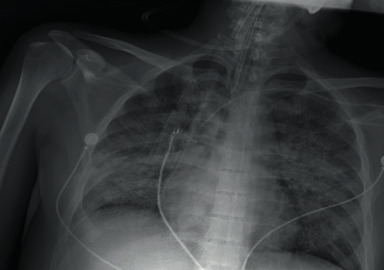
Introduction: Infection with SARS-CoV-2 increases the risk of acute graft dysfunction (AGD) in renal transplant recipients (RTR), and the risk of concurrently presenting with opportunistic infections is also increased. There is no current consensus on the management of immunosuppression during SARS-CoV-2 infection in RTR. Case Presentation. A 35-year-old male RTR from a living related donor presented with SARS-CoV-2 infection (January 2021). Two months later, despite alterations to his immunosuppression regimen (tacrolimus (TAC) was reduced by 50%, and the mycophenolic acid (MMF) was suspended with the remission of symptoms), the patient presented with pulmonary tuberculosis, pneumonia due to respiratory syncytial virus (RSV), cytomegalovirus (CMV) pneumonitis, and histoplasmosis (HP). Management was initiated with antituberculosis medications, ganciclovir, antibiotics, and liposomal amphotericin B, and the immunosuppressants were suspended, yet the patient's evolution was catastrophic and the outcome fatal.
Conclusion: We recommend that in RTR post-COVID-19, the immunosuppression regimen should be gradually reinstated along with strict vigilance in observing for highly prevalent coinfections (TB, HP, and CMV).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


