Fred H Geisler, Paul C McAfee, Robert J Banco, Scott L Blumenthal, Richard D Guyer, Richard T Holt, Mohamed E Majd
{"title":"CHARITÉ人工椎间盘与腰椎融合的前瞻性、随机、多中心FDA IDE研究:既往手术和既往椎间盘切除术对腰椎关节置换术后临床结果的5年随访影响","authors":"Fred H Geisler, Paul C McAfee, Robert J Banco, Scott L Blumenthal, Richard D Guyer, Richard T Holt, Mohamed E Majd","doi":"10.1016/SASJ-2008-0019-RR","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Candidates for spinal arthrodesis or arthroplasty often present with a history of prior surgery such as laminectomy, laminotomy or discectomy. In this study, lumbar arthroplasty patients with prior surgery, and in particular patients with prior discectomy, were evaluated for their clinical outcomes at the 5-year time point.</p><p><strong>Methods: </strong>Randomized patients from the 5-year CHARITÉ investigational device exemption (IDE) study were divided as follows: 1) fusion prior surgery (excluding prior decompression with fusion) group (FSG); 2) fusion prior discectomy group (FDG); 3) fusion no prior surgery group (FNG); 4) arthroplasty prior surgery group (ASG); 5) arthroplasty prior discectomy group (ADG); and 6) arthroplasty no prior surgery group (ANG). The 5-year clinical outcomes included visual analog scale (VAS), Oswestry Disability Index 2.0 (ODI), patient satisfaction, and work status.</p><p><strong>Results: </strong>In the arthroplasty group, all subgroups had statistically significant VAS improvements from baseline (VAS change from baseline: ASG = -36.6 ± 29.6, P < 0.0001; ADG = -40.2 ± 30.9, P = 0.0002; ANG = -36.5 ± 34.6, P < 0.0001). There was no statistical difference between subgroups (P = 0.5587). In the fusion group, VAS changes from baseline were statistically significant for the FNG and FSG subgroups, but not for the FDG patients (FNG = -46.3 ± 28.8, P < 0.0001; FSG = -24.2 ± 36.4, P = 0.0444; FDG = -26.7 ± 38.7, P = 0.2188). A trend of decreased VAS improvements was observed for FSG versus FNG (P = 0.0703) subgroups. Similar findings and trends were observed in ODI scores (Changes in ODI from baseline: ASG = -20.4 ± 23.8, P < 0.0001; ANG = -26.6±21.1, P < 0.0001; ADG= -17.6 ± 28.6, P = 0.0116; FSG = -14.5 ± 21.2, P = 0.0303; FNG= -32.5 ± 22.6, P < 0.0001; FDG = -10.7 ± 9.4, P = 0.0938). The greatest improvement in work status from preoperative to postoperative was seen in the ADG subgroup (28% increase in part- and full-time employment), while the FDG subgroup showed the greatest reduction in work status (17% decrease).</p><p><strong>Conclusions: </strong>Arthroplasty patients with prior surgery or prior discectomy had similar clinical outcomes as arthroplasty patients without prior surgery, while fusion patients with prior surgery or prior discectomy showed trends of lowered clinical outcomes compared to fusion patients without prior surgery or discectomy.</p>","PeriodicalId":88695,"journal":{"name":"SAS journal","volume":"3 1","pages":"17-25"},"PeriodicalIF":0.0000,"publicationDate":"2009-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/98/c9/SAS-3-2008-0019-RR.PMC4365588.pdf","citationCount":"4","resultStr":"{\"title\":\"Prospective, Randomized, Multicenter FDA IDE Study of CHARITÉ Artificial Disc versus Lumbar Fusion: Effect at 5-year Follow-up of Prior Surgery and Prior Discectomy on Clinical Outcomes Following Lumbar Arthroplasty.\",\"authors\":\"Fred H Geisler, Paul C McAfee, Robert J Banco, Scott L Blumenthal, Richard D Guyer, Richard T Holt, Mohamed E Majd\",\"doi\":\"10.1016/SASJ-2008-0019-RR\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Candidates for spinal arthrodesis or arthroplasty often present with a history of prior surgery such as laminectomy, laminotomy or discectomy. In this study, lumbar arthroplasty patients with prior surgery, and in particular patients with prior discectomy, were evaluated for their clinical outcomes at the 5-year time point.</p><p><strong>Methods: </strong>Randomized patients from the 5-year CHARITÉ investigational device exemption (IDE) study were divided as follows: 1) fusion prior surgery (excluding prior decompression with fusion) group (FSG); 2) fusion prior discectomy group (FDG); 3) fusion no prior surgery group (FNG); 4) arthroplasty prior surgery group (ASG); 5) arthroplasty prior discectomy group (ADG); and 6) arthroplasty no prior surgery group (ANG). The 5-year clinical outcomes included visual analog scale (VAS), Oswestry Disability Index 2.0 (ODI), patient satisfaction, and work status.</p><p><strong>Results: </strong>In the arthroplasty group, all subgroups had statistically significant VAS improvements from baseline (VAS change from baseline: ASG = -36.6 ± 29.6, P < 0.0001; ADG = -40.2 ± 30.9, P = 0.0002; ANG = -36.5 ± 34.6, P < 0.0001). There was no statistical difference between subgroups (P = 0.5587). In the fusion group, VAS changes from baseline were statistically significant for the FNG and FSG subgroups, but not for the FDG patients (FNG = -46.3 ± 28.8, P < 0.0001; FSG = -24.2 ± 36.4, P = 0.0444; FDG = -26.7 ± 38.7, P = 0.2188). A trend of decreased VAS improvements was observed for FSG versus FNG (P = 0.0703) subgroups. Similar findings and trends were observed in ODI scores (Changes in ODI from baseline: ASG = -20.4 ± 23.8, P < 0.0001; ANG = -26.6±21.1, P < 0.0001; ADG= -17.6 ± 28.6, P = 0.0116; FSG = -14.5 ± 21.2, P = 0.0303; FNG= -32.5 ± 22.6, P < 0.0001; FDG = -10.7 ± 9.4, P = 0.0938). The greatest improvement in work status from preoperative to postoperative was seen in the ADG subgroup (28% increase in part- and full-time employment), while the FDG subgroup showed the greatest reduction in work status (17% decrease).</p><p><strong>Conclusions: </strong>Arthroplasty patients with prior surgery or prior discectomy had similar clinical outcomes as arthroplasty patients without prior surgery, while fusion patients with prior surgery or prior discectomy showed trends of lowered clinical outcomes compared to fusion patients without prior surgery or discectomy.</p>\",\"PeriodicalId\":88695,\"journal\":{\"name\":\"SAS journal\",\"volume\":\"3 1\",\"pages\":\"17-25\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2009-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/98/c9/SAS-3-2008-0019-RR.PMC4365588.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAS journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/SASJ-2008-0019-RR\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2009/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAS journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/SASJ-2008-0019-RR","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2009/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Prospective, Randomized, Multicenter FDA IDE Study of CHARITÉ Artificial Disc versus Lumbar Fusion: Effect at 5-year Follow-up of Prior Surgery and Prior Discectomy on Clinical Outcomes Following Lumbar Arthroplasty.
Background: Candidates for spinal arthrodesis or arthroplasty often present with a history of prior surgery such as laminectomy, laminotomy or discectomy. In this study, lumbar arthroplasty patients with prior surgery, and in particular patients with prior discectomy, were evaluated for their clinical outcomes at the 5-year time point.
Methods: Randomized patients from the 5-year CHARITÉ investigational device exemption (IDE) study were divided as follows: 1) fusion prior surgery (excluding prior decompression with fusion) group (FSG); 2) fusion prior discectomy group (FDG); 3) fusion no prior surgery group (FNG); 4) arthroplasty prior surgery group (ASG); 5) arthroplasty prior discectomy group (ADG); and 6) arthroplasty no prior surgery group (ANG). The 5-year clinical outcomes included visual analog scale (VAS), Oswestry Disability Index 2.0 (ODI), patient satisfaction, and work status.
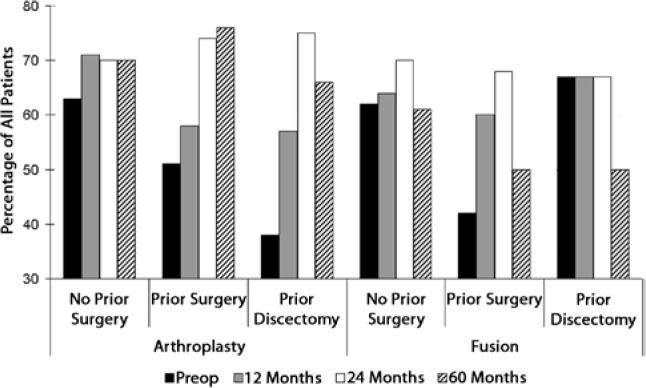
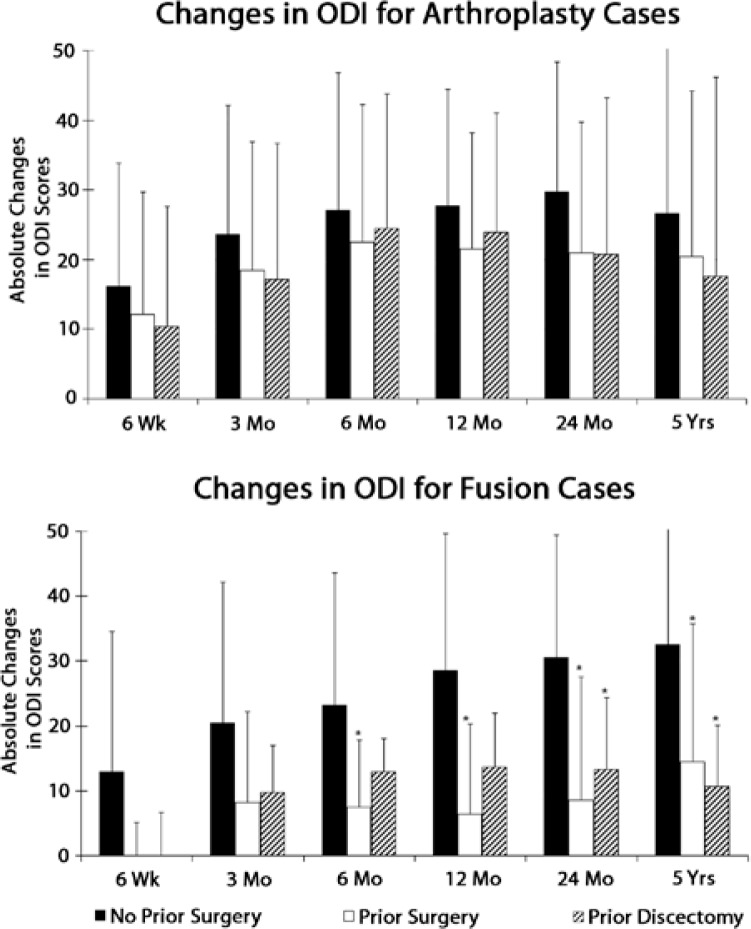
Results: In the arthroplasty group, all subgroups had statistically significant VAS improvements from baseline (VAS change from baseline: ASG = -36.6 ± 29.6, P < 0.0001; ADG = -40.2 ± 30.9, P = 0.0002; ANG = -36.5 ± 34.6, P < 0.0001). There was no statistical difference between subgroups (P = 0.5587). In the fusion group, VAS changes from baseline were statistically significant for the FNG and FSG subgroups, but not for the FDG patients (FNG = -46.3 ± 28.8, P < 0.0001; FSG = -24.2 ± 36.4, P = 0.0444; FDG = -26.7 ± 38.7, P = 0.2188). A trend of decreased VAS improvements was observed for FSG versus FNG (P = 0.0703) subgroups. Similar findings and trends were observed in ODI scores (Changes in ODI from baseline: ASG = -20.4 ± 23.8, P < 0.0001; ANG = -26.6±21.1, P < 0.0001; ADG= -17.6 ± 28.6, P = 0.0116; FSG = -14.5 ± 21.2, P = 0.0303; FNG= -32.5 ± 22.6, P < 0.0001; FDG = -10.7 ± 9.4, P = 0.0938). The greatest improvement in work status from preoperative to postoperative was seen in the ADG subgroup (28% increase in part- and full-time employment), while the FDG subgroup showed the greatest reduction in work status (17% decrease).
Conclusions: Arthroplasty patients with prior surgery or prior discectomy had similar clinical outcomes as arthroplasty patients without prior surgery, while fusion patients with prior surgery or prior discectomy showed trends of lowered clinical outcomes compared to fusion patients without prior surgery or discectomy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


