Shyam K Tanguturi, Ming-Hui Chen, Marian Loffredo, Jerome P Richie, Anthony V D'Amico
{"title":"评估PSA作为保留神经的根治性前列腺切除术的选择标准的影响。","authors":"Shyam K Tanguturi, Ming-Hui Chen, Marian Loffredo, Jerome P Richie, Anthony V D'Amico","doi":"10.1155/2014/395078","DOIUrl":null,"url":null,"abstract":"<p><p>Purpose. We investigated whether NS-RP increased risk of PSA failure and whether PSA should be included as a selection criterion for NS. Methods. We evaluated 357 consecutive men with screen-detected PC who underwent open RP without adjuvant radiotherapy between 9/11/2001 and 12/30/2008. Criteria for NS included Gleason score ≤3 + 4, percentage of positive biopsies (PPB) ≤50%, percentage of core involvement ≤50%, nonapical location, no perineural invasion, and no palpable disease on pre- or intraoperative exam but did not include a PSA threshold. Cox multivariable regression assessed whether increasing PSA or unilateral- or bilateral-NS versus non-NS-RP was associated with PSA failure adjusting for prognostic factors. Results. After a median follow-up of 3.96 years, 34 men sustained PSA failure (9.5%). Increasing PSA was significantly associated with increased risk of PSA failure in the interaction model (adjusted hazard ratio (AHR): 1.09 [95% CI: 1.03-1.16]; P = 0.005), whereas unilateral (AHR: 1.24 [95% CI: 0.36-4.34]; P = 0.73) or bilateral NS (AHR: 0.41 [95% CI: 0.06-2.59]; P = 0.34) versus non-NS RP was not. Conclusion. NS-RP in a screened cohort did not increase risk of PSA failure using NS criteria not including PSA. </p>","PeriodicalId":20907,"journal":{"name":"Prostate Cancer","volume":"2014 ","pages":"395078"},"PeriodicalIF":2.0000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/395078","citationCount":"5","resultStr":"{\"title\":\"Evaluating the Impact of PSA as a Selection Criteria for Nerve Sparing Radical Prostatectomy in a Screened Cohort.\",\"authors\":\"Shyam K Tanguturi, Ming-Hui Chen, Marian Loffredo, Jerome P Richie, Anthony V D'Amico\",\"doi\":\"10.1155/2014/395078\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Purpose. We investigated whether NS-RP increased risk of PSA failure and whether PSA should be included as a selection criterion for NS. Methods. We evaluated 357 consecutive men with screen-detected PC who underwent open RP without adjuvant radiotherapy between 9/11/2001 and 12/30/2008. Criteria for NS included Gleason score ≤3 + 4, percentage of positive biopsies (PPB) ≤50%, percentage of core involvement ≤50%, nonapical location, no perineural invasion, and no palpable disease on pre- or intraoperative exam but did not include a PSA threshold. Cox multivariable regression assessed whether increasing PSA or unilateral- or bilateral-NS versus non-NS-RP was associated with PSA failure adjusting for prognostic factors. Results. After a median follow-up of 3.96 years, 34 men sustained PSA failure (9.5%). Increasing PSA was significantly associated with increased risk of PSA failure in the interaction model (adjusted hazard ratio (AHR): 1.09 [95% CI: 1.03-1.16]; P = 0.005), whereas unilateral (AHR: 1.24 [95% CI: 0.36-4.34]; P = 0.73) or bilateral NS (AHR: 0.41 [95% CI: 0.06-2.59]; P = 0.34) versus non-NS RP was not. Conclusion. NS-RP in a screened cohort did not increase risk of PSA failure using NS criteria not including PSA. </p>\",\"PeriodicalId\":20907,\"journal\":{\"name\":\"Prostate Cancer\",\"volume\":\"2014 \",\"pages\":\"395078\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2014-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2014/395078\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Prostate Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2014/395078\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/395078","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Evaluating the Impact of PSA as a Selection Criteria for Nerve Sparing Radical Prostatectomy in a Screened Cohort.
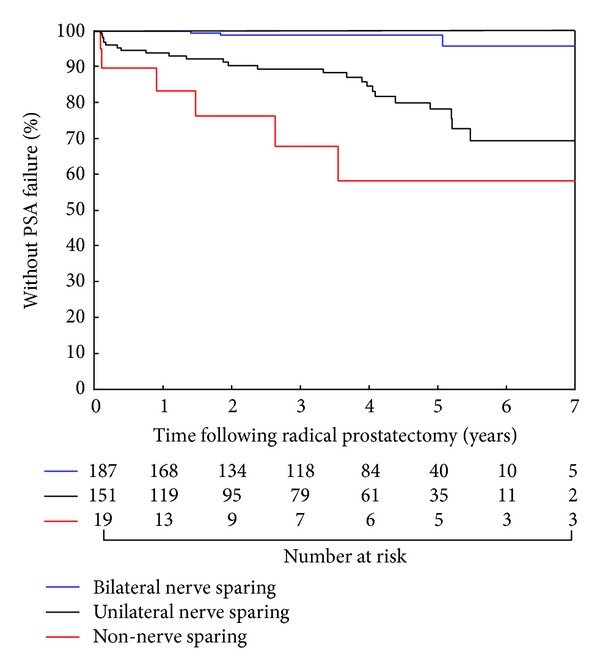
Purpose. We investigated whether NS-RP increased risk of PSA failure and whether PSA should be included as a selection criterion for NS. Methods. We evaluated 357 consecutive men with screen-detected PC who underwent open RP without adjuvant radiotherapy between 9/11/2001 and 12/30/2008. Criteria for NS included Gleason score ≤3 + 4, percentage of positive biopsies (PPB) ≤50%, percentage of core involvement ≤50%, nonapical location, no perineural invasion, and no palpable disease on pre- or intraoperative exam but did not include a PSA threshold. Cox multivariable regression assessed whether increasing PSA or unilateral- or bilateral-NS versus non-NS-RP was associated with PSA failure adjusting for prognostic factors. Results. After a median follow-up of 3.96 years, 34 men sustained PSA failure (9.5%). Increasing PSA was significantly associated with increased risk of PSA failure in the interaction model (adjusted hazard ratio (AHR): 1.09 [95% CI: 1.03-1.16]; P = 0.005), whereas unilateral (AHR: 1.24 [95% CI: 0.36-4.34]; P = 0.73) or bilateral NS (AHR: 0.41 [95% CI: 0.06-2.59]; P = 0.34) versus non-NS RP was not. Conclusion. NS-RP in a screened cohort did not increase risk of PSA failure using NS criteria not including PSA.
期刊介绍:
Prostate Cancer is a peer-reviewed, Open Access journal that provides a multidisciplinary platform for scientists, surgeons, oncologists and clinicians working on prostate cancer. The journal publishes original research articles, review articles, and clinical studies related to the diagnosis, surgery, radiotherapy, drug discovery and medical management of the disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


