Antonio Gómez-Outes, Ana Isabel Terleira-Fernández, Gonzalo Calvo-Rojas, M Luisa Suárez-Gea, Emilio Vargas-Castrillón
{"title":"达比加群、利伐沙班或阿哌沙班与华法林对非瓣膜性心房颤动患者的影响:一项系统综述和亚组荟萃分析","authors":"Antonio Gómez-Outes, Ana Isabel Terleira-Fernández, Gonzalo Calvo-Rojas, M Luisa Suárez-Gea, Emilio Vargas-Castrillón","doi":"10.1155/2013/640723","DOIUrl":null,"url":null,"abstract":"<p><p>Background. New oral anticoagulants (NOAC; rivaroxaban, dabigatran, apixaban) have become available as an alternative to warfarin anticoagulation in non-valvular atrial fibrillation (NVAF). Methods. MEDLINE and CENTRAL, regulatory agencies websites, clinical trials registers and conference proceedings were searched to identify randomised controlled trials of NOAC versus warfarin in NVAF. Two investigators reviewed all studies and extracted data on patient and study characteristics along with cardiovascular outcomes. Relative risks (RR) and 95% confidence intervals (CI) were estimated using a random effect meta-analysis. Results. Three clinical trials in 50,578 patients were included. The risk of non-hemorrhagic stroke and systemic embolic events (SEE) was similar with the NOAC and warfarin (RR = 0.93; 95% CI = 0.83-1.04), while the risk of intracranial bleeding (ICB) with the NOAC was lower than with warfarin (RR = 0.46; 95% CI = 0.33-0.65). We found differences in the effect size on all strokes and SEE depending on geographic region as well as on non-hemorrhagic stroke, SEE, bleeding and mortality depending on time in therapeutic range. Conclusion. The NOAC seem no more effective than warfarin for prevention of nonhemorrhagic stroke and SEE in the overall NVAF population, but are generally associated with a lower risk of ICB than warfarin. </p>","PeriodicalId":75222,"journal":{"name":"Thrombosis","volume":"2013 ","pages":"640723"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/640723","citationCount":"173","resultStr":"{\"title\":\"Dabigatran, Rivaroxaban, or Apixaban versus Warfarin in Patients with Nonvalvular Atrial Fibrillation: A Systematic Review and Meta-Analysis of Subgroups.\",\"authors\":\"Antonio Gómez-Outes, Ana Isabel Terleira-Fernández, Gonzalo Calvo-Rojas, M Luisa Suárez-Gea, Emilio Vargas-Castrillón\",\"doi\":\"10.1155/2013/640723\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Background. New oral anticoagulants (NOAC; rivaroxaban, dabigatran, apixaban) have become available as an alternative to warfarin anticoagulation in non-valvular atrial fibrillation (NVAF). Methods. MEDLINE and CENTRAL, regulatory agencies websites, clinical trials registers and conference proceedings were searched to identify randomised controlled trials of NOAC versus warfarin in NVAF. Two investigators reviewed all studies and extracted data on patient and study characteristics along with cardiovascular outcomes. Relative risks (RR) and 95% confidence intervals (CI) were estimated using a random effect meta-analysis. Results. Three clinical trials in 50,578 patients were included. The risk of non-hemorrhagic stroke and systemic embolic events (SEE) was similar with the NOAC and warfarin (RR = 0.93; 95% CI = 0.83-1.04), while the risk of intracranial bleeding (ICB) with the NOAC was lower than with warfarin (RR = 0.46; 95% CI = 0.33-0.65). We found differences in the effect size on all strokes and SEE depending on geographic region as well as on non-hemorrhagic stroke, SEE, bleeding and mortality depending on time in therapeutic range. Conclusion. The NOAC seem no more effective than warfarin for prevention of nonhemorrhagic stroke and SEE in the overall NVAF population, but are generally associated with a lower risk of ICB than warfarin. </p>\",\"PeriodicalId\":75222,\"journal\":{\"name\":\"Thrombosis\",\"volume\":\"2013 \",\"pages\":\"640723\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2013/640723\",\"citationCount\":\"173\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thrombosis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2013/640723\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/12/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thrombosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/640723","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/12/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 173
摘要
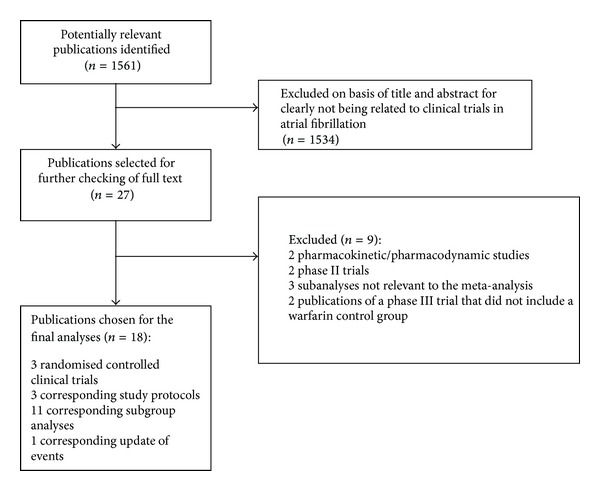
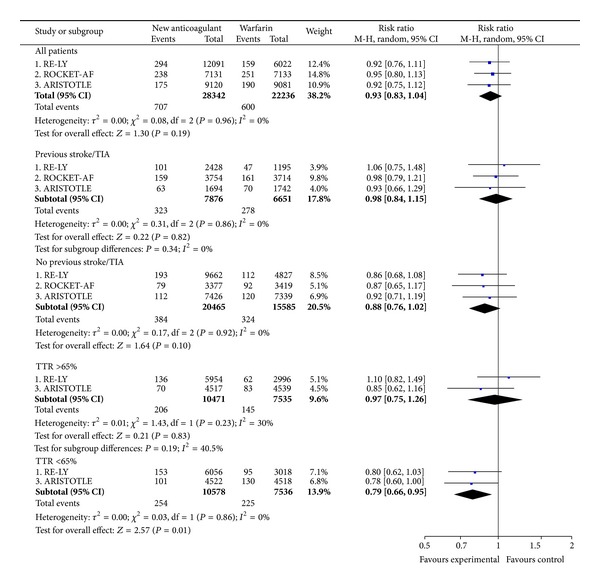
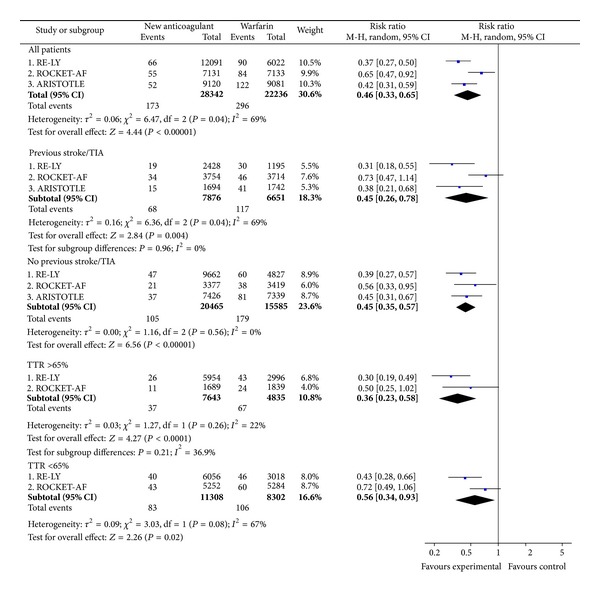
背景。新型口服抗凝剂;利伐沙班,达比加群,阿哌沙班)已成为华法林抗凝治疗非瓣膜性心房颤动(NVAF)的替代药物。方法。我们检索了MEDLINE和CENTRAL、监管机构网站、临床试验注册和会议记录,以确定NOAC与华法林在非瓣瓣性房颤中的随机对照试验。两位研究者回顾了所有的研究,并提取了患者和研究特征以及心血管结果的数据。使用随机效应荟萃分析估计相对风险(RR)和95%置信区间(CI)。结果。3项临床试验纳入50,578例患者。非出血性卒中和系统性栓塞事件(SEE)的风险与NOAC和华法林相似(RR = 0.93;95% CI = 0.83-1.04),而NOAC组颅内出血(ICB)的风险低于华法林组(RR = 0.46;95% ci = 0.33-0.65)。我们发现所有中风和SEE的效应大小取决于地理区域,以及非出血性中风、SEE、出血和死亡率取决于治疗范围内的时间。结论。在所有非瓣膜性房颤人群中,NOAC似乎并不比华法林更有效地预防非出血性卒中和SEE,但通常与华法林相比,其ICB风险较低。
Dabigatran, Rivaroxaban, or Apixaban versus Warfarin in Patients with Nonvalvular Atrial Fibrillation: A Systematic Review and Meta-Analysis of Subgroups.
Background. New oral anticoagulants (NOAC; rivaroxaban, dabigatran, apixaban) have become available as an alternative to warfarin anticoagulation in non-valvular atrial fibrillation (NVAF). Methods. MEDLINE and CENTRAL, regulatory agencies websites, clinical trials registers and conference proceedings were searched to identify randomised controlled trials of NOAC versus warfarin in NVAF. Two investigators reviewed all studies and extracted data on patient and study characteristics along with cardiovascular outcomes. Relative risks (RR) and 95% confidence intervals (CI) were estimated using a random effect meta-analysis. Results. Three clinical trials in 50,578 patients were included. The risk of non-hemorrhagic stroke and systemic embolic events (SEE) was similar with the NOAC and warfarin (RR = 0.93; 95% CI = 0.83-1.04), while the risk of intracranial bleeding (ICB) with the NOAC was lower than with warfarin (RR = 0.46; 95% CI = 0.33-0.65). We found differences in the effect size on all strokes and SEE depending on geographic region as well as on non-hemorrhagic stroke, SEE, bleeding and mortality depending on time in therapeutic range. Conclusion. The NOAC seem no more effective than warfarin for prevention of nonhemorrhagic stroke and SEE in the overall NVAF population, but are generally associated with a lower risk of ICB than warfarin.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


