Max Mifsud, Jamie Y Ferguson, David A Stubbs, Alex J Ramsden, Martin A McNally
{"title":"同时清创,Ilizarov重建和游离肌瓣治疗复杂胫骨感染。","authors":"Max Mifsud, Jamie Y Ferguson, David A Stubbs, Alex J Ramsden, Martin A McNally","doi":"10.5194/jbji-6-63-2020","DOIUrl":null,"url":null,"abstract":"<p><p>Chronic bone infections often present with complex bone and soft tissue loss. Management is difficult and commonly delivered in multiple stages over many months. This study investigated the feasibility and clinical outcomes of reconstruction in one stage. Fifty-seven consecutive patients with chronic osteomyelitis ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>27</mn></mrow> </math> ) or infected non-union ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>30</mn></mrow> </math> ) were treated with simultaneous debridement, Ilizarov method and free muscle flap transfer. 41 patients (71.9 %) had systemic co-morbidities (Cierny-Mader group Bs hosts). Infection was confirmed with strict criteria. 48 patients (84.2 %) had segmental defects. The primary outcome was eradication of infection at final follow-up. Secondary outcomes included bone union, flap survival and complications or re-operation related to the reconstruction. Infection was eradicated in <math><mrow><mn>55</mn> <mo>/</mo> <mn>57</mn></mrow> </math> cases (96.5 %) at a mean follow-up of 36 months (range 12-146). No flap failures occurred during distraction but 6 required early anastomotic revision and 3 were not salvageable (flap failure rate 5.3 %). Bony union was achieved in <math><mrow><mn>52</mn> <mo>/</mo> <mn>57</mn></mrow> </math> (91.2 %) with the initial surgery alone. After treatment of the five un-united docking sites, all cases achieved bony union at final follow-up. Simultaneous reconstruction with Ilizarov method and free tissue transfer is safe but requires careful planning and logistic considerations. The outcomes from this study are equivalent or better than those reported after staged surgery.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"6 3","pages":"63-72"},"PeriodicalIF":2.8000,"publicationDate":"2020-12-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7852407/pdf/","citationCount":"7","resultStr":"{\"title\":\"Simultaneous debridement, Ilizarov reconstruction and free muscle flaps in the management of complex tibial infection.\",\"authors\":\"Max Mifsud, Jamie Y Ferguson, David A Stubbs, Alex J Ramsden, Martin A McNally\",\"doi\":\"10.5194/jbji-6-63-2020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Chronic bone infections often present with complex bone and soft tissue loss. Management is difficult and commonly delivered in multiple stages over many months. This study investigated the feasibility and clinical outcomes of reconstruction in one stage. Fifty-seven consecutive patients with chronic osteomyelitis ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>27</mn></mrow> </math> ) or infected non-union ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>30</mn></mrow> </math> ) were treated with simultaneous debridement, Ilizarov method and free muscle flap transfer. 41 patients (71.9 %) had systemic co-morbidities (Cierny-Mader group Bs hosts). Infection was confirmed with strict criteria. 48 patients (84.2 %) had segmental defects. The primary outcome was eradication of infection at final follow-up. Secondary outcomes included bone union, flap survival and complications or re-operation related to the reconstruction. Infection was eradicated in <math><mrow><mn>55</mn> <mo>/</mo> <mn>57</mn></mrow> </math> cases (96.5 %) at a mean follow-up of 36 months (range 12-146). No flap failures occurred during distraction but 6 required early anastomotic revision and 3 were not salvageable (flap failure rate 5.3 %). Bony union was achieved in <math><mrow><mn>52</mn> <mo>/</mo> <mn>57</mn></mrow> </math> (91.2 %) with the initial surgery alone. After treatment of the five un-united docking sites, all cases achieved bony union at final follow-up. Simultaneous reconstruction with Ilizarov method and free tissue transfer is safe but requires careful planning and logistic considerations. The outcomes from this study are equivalent or better than those reported after staged surgery.</p>\",\"PeriodicalId\":15271,\"journal\":{\"name\":\"Journal of Bone and Joint Infection\",\"volume\":\"6 3\",\"pages\":\"63-72\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2020-12-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7852407/pdf/\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Joint Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5194/jbji-6-63-2020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-6-63-2020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Simultaneous debridement, Ilizarov reconstruction and free muscle flaps in the management of complex tibial infection.
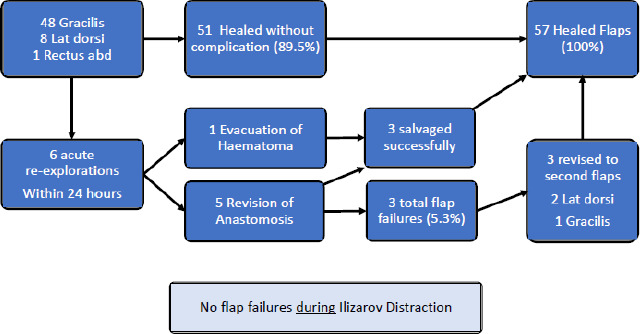
Chronic bone infections often present with complex bone and soft tissue loss. Management is difficult and commonly delivered in multiple stages over many months. This study investigated the feasibility and clinical outcomes of reconstruction in one stage. Fifty-seven consecutive patients with chronic osteomyelitis ( ) or infected non-union ( ) were treated with simultaneous debridement, Ilizarov method and free muscle flap transfer. 41 patients (71.9 %) had systemic co-morbidities (Cierny-Mader group Bs hosts). Infection was confirmed with strict criteria. 48 patients (84.2 %) had segmental defects. The primary outcome was eradication of infection at final follow-up. Secondary outcomes included bone union, flap survival and complications or re-operation related to the reconstruction. Infection was eradicated in cases (96.5 %) at a mean follow-up of 36 months (range 12-146). No flap failures occurred during distraction but 6 required early anastomotic revision and 3 were not salvageable (flap failure rate 5.3 %). Bony union was achieved in (91.2 %) with the initial surgery alone. After treatment of the five un-united docking sites, all cases achieved bony union at final follow-up. Simultaneous reconstruction with Ilizarov method and free tissue transfer is safe but requires careful planning and logistic considerations. The outcomes from this study are equivalent or better than those reported after staged surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


