{"title":"第25卷:总统讲话:20世纪的男科学:对我们过去25年进步的评论","authors":"Gail S. Prins, William Bremner","doi":"10.1002/j.1939-4640.2004.tb02812.x","DOIUrl":null,"url":null,"abstract":"<p>In a heartbeat, we are there. Twenty-five years ago, Dr Nancy Alexander, President of the American Society of Andrology (ASA), delivered a Presidential Address at the 1980 ASA Annual Meeting in Chicago where she shared with us her perceptions for the future of andrology by the year 2000. This “state-of-the-art” address, titled “Andrology in the Year 2000,” was published in its entirety in the first volume of the <i>Journal of Andrology</i> (<i>J Androl</i>. 1980;1:149–157). It's a wonderful set of predictions, and we encourage our readers to go back to this manuscript and read (or reread) her insightful comments made at a time when the field of andrology was relatively new. The focus of Dr Alexander's comments and predictions for the year 2000 was not the entire field of andrology, but rather, 2 facets that are her area of expertise: 1) advances in male contraception, and 2) basic and clinical studies on development and maintenance of male fertility. In celebration of the Silver Anniversary of the <i>Journal of Andrology</i>, the 2004 ASA Presidents now reflect on Dr Alexander's comments and describe how the subsequent events during the past 25 years have confirmed or changed her predictions for andrology in the year 2000.</p><p>In 1978, National Institutes of Health (NIH) funding for population research had grown considerably from the previous 15 years and reached a total of $112 million set aside for the year. The ratio of male-female reproductive system funding was approximately 1:2, which was a vast improvement over the 1:4 ratio in 1972 (Alexander, 1980). The future for male reproductive research was promising. To address the current status of NIH funding for reproductive research, we asked the National Institute of Child Health and Human Development (NICHD) of the NIH to provide data on their funding levels during the past 5 years (1999–2003) in the areas of male and female reproductive research. It is important to stress that these numbers reflect NICHD funding only and do not include male reproductive system research by other institutes such as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the National Institute on Aging (NIA), and the National Institute of Environmental Health Sciences (NIEHS), all of which have research programs that include the male reproductive tract. Nonetheless, the NICHD is considered the primary institute for reproductive research and can be used as an indicator of fiscal commitments to reproductive research. Three categories were defined for analysis and are shown in the Figure: 1) targeted male reproductive health (research that applies only to male reproductive health [eg, endocrine regulation of germ cell apoptosis in the male, examinations of male fertility, Sertoli cell development]), 2) targeted female reproductive health (research that applies only to female reproductive health [eg, gonadotropin secretion during lactation, progestin regulation of uterine hemostasis and angiogenesis, prevalence and etiologic predictors of vulvodynia]), and 3) research applicable to both male and female reproductive health and not included in categories 1 or 2 (eg, sperm—egg interactions, human immunodeficiency virus [HIV] prevention methods, efficacy of infertility treatments). Data collected for these 3 categories between 1992 and 1998 indicated a steady funding level at a 1:2 ratio for male-female targeted research, as it was in 1978. With the concerted effort to double the NIH budget between 1998 and 2002, there was a marked increase in research funding in all 3 categories (Figure). That's the good (great) news. The bad news is that funding increases in male reproductive health research lagged behind those for female (category 2) and male and female (category 3) reproductive health research, bringing the simplistic male-female research ratio close to 1:4 again, the value in 1972. Explanations for the disparate funding increases are multifactorial and include the initiation of the Women's Reproductive Health Research career development programs and the NICHD's collaboration with the Office of Women's Health to administer the “Building Interdisciplinary Research in Women's Health.” Nonetheless, it is disheartening to see a return to greater disparity between male and female reproductive health emphasis at the NICHD rather than the reduced disparity predicted by Dr Alexander 25 years ago. Several key factors also contributed to the increased level of funding for research that is applicable to both male and female reproductive health during the past 5 years. For instance, the NICHD is now supporting the development and operation of a Biological Testing Facility and a Peptide Synthesis Facility. These facilities help researchers develop and assess the potential clinical uses of new compounds and formulations. Another contributing factor is that the NICHD has taken the opportunity to fund research under Center Core Grants that the National Institute of Allergy and Infectious Diseases manages. All of these activities include research applicable to male reproductive health, so there is optimism in these numbers as well. We hope that the expected downturn in NIH funding levels during the next several years will not too negatively affect the field of andrology.</p><p>Dr Alexander mentioned several aspects of the hormonal control of human spermatogenesis and the initial approaches to contraception using endocrine (steroid) administration. She predicted that by 2000, we would not have a male pill but that potential products would be undergoing testing. Both of these predictions have proven correct. However, she predicted that the approaches being tested in the early years of the new millennium would not be steroids. This prediction was not correct; all the major trials in recent years have involved steroids, particularly regimens combining an androgen (various forms of testosterone) and progestins (such as desogestrel, levonorgestrel, depot medroxyprogesterone acetate, norethisterone enanthate). Such regimens are now quite effective; the pharmaceutical industry (at least in Europe) has taken notice, and a multicenter trial, sponsored by Organon and Schering, is under way using testosterone undecanoate and 3-keto desogestrel. Unfortunately, the planned participation by 2 US centers in this study was prevented by the Food and Drug Administration, which is requiring additional animal data. Dr Alexander suggested that superactive analogs of gonadotropin-releasing hormone (GnRH) combined with testosterone would provide adequate spermatogenic suppression. This approach has been disappointing, but the possible utility of antagonist analogs of GnRH, particularly in induction regimens, is under active investigation in combination regimens with various testosterone compounds and formulations.</p><p>The prediction of Dr Alexander that, by 2000, we would be closer to an immunologic method of preventing male fertility has not proven to be correct. These approaches have foundered on difficulties with reliable induction of fertility suppression, unpredictable return to fertility, and adverse side effects. No such technique is in clinical trials, nor are animal studies particularly promising. Substantially greater understanding of the basic control mechanisms of immunology will be required prior to readdressing the clinical application of immunologic approaches.</p><p>Finally, Dr Alexander's own findings of increased atherosclerotic disease following vasectomy in animals have not been confirmed in extensive studies of men. Therefore, her prediction that this putative complication would decrease the numbers of vasectomies has not been borne out by subsequent clinical experience. Vasectomy remains a very effective, safe, and widely used method for permanent fertility control in men.</p><p>Extensive research on the epididymis has been conducted during the past quarter century, and several of the issues addressed by Dr Alexander with regard to epididymal function, protein secretions, and histology are beginning to be unraveled. For example, one set of experiments has shown the importance of the initial segment, at least in mice. Knockouts of the orphan tyrosine kinase receptor c-Ros show an undeveloped initial segment and male infertility (Sonnenberg-Riethmacher et al, 1996). The infertility defect appears to be due to a defect in tail angulation, and thus, the sperm fail to reach the egg. Tantalizing evidence suggests that the infertility phenotype is due to the failure of sperm to regulate their cell volume, which may be due to an altered epididymal luminal fluid microenvironment (Yeung et al, 2000). In 1980, although a few components of epididymal secretions had been identified, we had no idea about their role in sperm maturation, their maintenance during storage, or their activity after ejaculation. Scientists now have some evidence-based ideas. One current hypothesis is that organic solutes secreted into the epididymal lumen are osmolytes that regulate water movement into and out of both sperm and epididymal epithelial cells, similar to their role in the kidney. That solutes such as inositol, <span>l</span>-carnitine, glycerophosphorylcholine, and glutamate are found in the 50–60 mmol/L range (Hinton and Palladino, 1995) lends support for this role. Furthermore, osmolytes may protect sperm cells from rapid changes in osmolarity, which is important, since epididymal luminal fluid is hyperosmotic.</p><p>In 1980, Dr Alexander stated that “Only initial studies have been done on the various protein components… of the epididymal secretions” and predicted that their identification would eventually lead to new treatment methods for infertility. Following the revolution in molecular biology, this is currently the most studied aspect of epididymal biology, and many proteins have been recently discovered. While some proteins are unique to the epididymis, others are ubiquitous. The challenge to uncover their role(s) remains, since only a few secreted proteins have been assigned some kind of function. For example, the epididymis secretes defensins and defensin-like molecules, presumably for the protection of sperm and the epididymis itself (Von Horsten et al, 2002; Rao et al, 2003). CRISP-1 is a secreted protein that may be involved in either capacitation or sperm—egg binding (Cohen et al, 2000; Roberts et al, 2003). Other proteins have been identified with a putative function (eg, proteases, protease inhibitors, other enzymes), but again, their role in sperm maturation (if indeed there is one) is unknown. One recent leap forward is the identification of transporters in both sperm and epididymal epithelial cells, which has helped researchers understand how the epididymis forms the specialized luminal fluid environment. For example, several water, ion, and organic solute transporters have been identified and include the aquaporins; hydrogen plus adenosine triphosphatase for hydrogen ion transport; NHE-RF, a transporter involved in sodium/bicarbonate transport; and OCTN2, which transports <span>l</span>-carnitine (Breton et al, 1998; Bagnis et al, 2001; Rodriguez et al, 2002; Cheung et al, 2003). It is likely that no single secretory component is responsible for sperm maturation, but rather, that this process involves a complex series or cascade of events involving multiple cell—cell interactions.</p><p>A call was made for the development of research tools for the localization of cellular components. Considerable advances have been made in this field, and more and more proteins have been localized in different epididymal cell types. With laser capture technology, it is now possible to capture individual epithelial cells and perform reverse transcriptase-polymerase chain reaction (Kirby et al, 2003), generate complementary DNA libraries, and perform gene arrays. Hence, it is predicted that, in a few years, we will have a more thorough idea of the function of each epididymal cell type. Nonetheless, we still lack an understanding of the fundamental cell biology of epididymal function—protein synthesis, trafficking, secretion, and endocytosis, for instance, and this remains an area of future need. With advances in imaging, we can now perform in situ hybridization with immunohistochemistry, observe calcium movements in real time, and track epididymal development and fluid movement with time-lapse microscopy; thus, further advances are on the horizon. With more gene promoters being analyzed, it will not be too long before it will be possible to target gene silencing agents to specific epididymal cell types, as is already done to some regions of the epididymis. Hence, these approaches may also provide valuable information on the function of some genes/proteins in a cell type in a particular epididymal region in the very near future.</p><p>Major advances were made during the past quarter century to standardize semen analysis within the andrology community. Andrology laboratories in the United States now are included under the Clinical Laboratory Improvement Act (CLIA), which considers semen analysis a high-complexity test. Among other regulations, this designation requires adherence to strict standards, including daily quality control, laboratory certification or accreditation with attendant inspections, and oversight of a board-certified, doctoral-level laboratory director. Consequently, proficiency testing is now available from many providers for sperm concentration, viability, morphology, antisperm antibody assessment, and, most recently, motility. This semiannual assessment demonstrates a laboratory's ability to accurately analyze these male reproductive measures. Changes to CLIA now include periodic technologist competency testing, which is commercially available.</p><p>The World Health Organization (WHO) <i>Laboratory Manual for the Examination of Human Semen</i> is now published in its 4th edition and, since 1980, has set performance and evaluation recommendations that are used worldwide (WHO, 1999). Although semen analysis standards were not published by the ASA as Dr Alexander thought appropriate, many current and past ASA members have been intimately involved in writing these and other guidelines with the worldwide community. That we are now working from the 4th edition speaks for the fact that semen analysis, like all laboratory testing, requires continuous updating and reevaluation. This is most apparent in the area of sperm morphology, where evaluation systems have changed markedly over the years. In fact, this past year at the 2004 ASA Annual Meeting, a full-day Sperm Morphology Workshop was held that focused on laboratory-based training of the 2 most popular sperm morphology classification systems used by fertility specialists today: the WHO 3rd edition and the WHO 4th edition, also known as Strict Criteria. Unfortunately, clear standards for these systems are lacking, making the reproducibility of analysis difficult. We continue to need consistency and training for the clinical laboratory as well as for toxicology and industrial studies, which are now mandated in the United States.</p><p>During the past 20 years, we witnessed the introduction and use of computer-assisted semen analysis (CASA) systems for sperm concentration and motility analysis in the clinical and research andrology laboratory. While broadening and quantifying our information on motility parameters, these CASA systems, when used correctly, can reduce subjective variability in semen analysis across technicians in a single laboratory and even between laboratories. However, useful clinical correlates for all of the new motility information are still lacking and remain an area of future research. The application of CASA to morphometric analysis of sperm is relatively new, and its use is hampered by a lack of clear morphology standards. The cost and complexity of most CASA instruments remain significant barriers to their widespread adoption.</p><p>The past 25 years have brought enormous advances and uses for andrology testing and application above and beyond what was anticipated by Dr Alexander or anyone else, for that matter. The Hamster Ova—Sperm Penetration Assay or SPA, introduced by Rogers (1985), became a standard tool for the comprehensive andrology laboratory as predicted. Throughout the 1980s and 1990s, the SPA was widely used for evaluating the fertilizing potential of human spermatozoa with a discriminating power greater than that of the semen analysis alone (Rogers, 1985). As predicted, this technology was marketed by several commercial ventures. Reference laboratories developed systems for overnight transportation of sperm samples, which allowed centralized laboratories to perform the SPA for clinicians across the country and made this test widely available. Additionally, several companies sold frozen hamster ova, which made offering this assay a possibility in andrology laboratories that did not have prior access to an animal facility. As in vitro fertilization (IVF) became common practice for achieving pregnancy in the infertile couple, the SPA proved to be predictive of fertilization success in vitro. However, with the advent of intracytoplasmic sperm injection (ICSI), the use of the SPA has waned considerably. Although this test was shown to be predicative of the need for ICSI (Gvakharia et al, 2000), the success of ICSI and its subsequent widespread use and application in almost every IVF clinic have rendered the labor-intensive and costly SPA obsolete.</p><p>It was predicted that cervical mucus penetration assays would become a routine andrology laboratory test and, indeed, this came to pass. This aided the physician in making choices for the use of artificial insemination or even sperm donor insemination when “hostile” mucus was encountered for the sperm from a female's partner. Antisperm antibody testing not only became standard in the andrology work-up but also highly specific with the introduction of the Immunobead Test, which identified the immunoglobulin subtype present on sperm or within the female genital tract (Carson et al, 1988). However, once again, with the commonplace use of IVF-ICSI for establishing pregnancies in the infertile couple, the use of both of these assays has waned considerably from their peak usage in the 1990s.</p><p>Newer andrology laboratory tests have been introduced during the past decade and, although not commonplace in the standard andrology laboratory, their availability in centralized reference laboratories has allowed their implementation when clinically necessary. The Sperm Chromatin Structure Assay assesses sperm DNA fragmentation and has been found to correlate with fertility potential (Evenson and Jost, 2000). In addition to its routine prognostic value, this cytometry assay is useful for evaluating men at increased risk for DNA damage that can follow occupational exposures, that can occur with aging, or that can follow freeze-thaw procedures. Discoveries in the field of genetics have led to Y-chromosome deletion testing for infertile men, and commercial kits are available for this purpose. Full deletions or microdeletions in the long arm of the Y chromosome (azoospermic factor or AZF regions) have been shown to cause azoospermia, oligozoospermia, and related male infertility problems, and the ability to screen for these in the infertile patient has vastly improved diagnostic capabilities (Kent-First et al, 1996; Reijo et al, 1996). The use of testicular sperm extraction (TESE) from azoospermic men, combined with IVF-ICSI to achieve fertilization, permits the transmission of Y-related infertility to the male offspring, making this testing modality imperative for informed decision making by the patients who undergo these procedures.</p><p>The past 25 years have seen the rise, as well as the subsequent decline, of intensive andrology testing in the work-up of the infertile couple. The ease and availability of assisted reproductive technologies (ART) have led many clinicians to implement these techniques quickly and to forgo a full diagnostic male evaluation. Although this approach may lead to a pregnancy in the short term, it carries the risk that the cause of infertility will go undiagnosed. Since infertility can be a marker of serious medical problems or toxicant exposures, denying the male partner a full work-up has important health consequences. Furthermore, several studies have shown that the cost-effectiveness (cost per live delivery) of treating more common male factor problems such as varicocele or vasal and/or epididymal obstruction is much greater than the initial use of IVF-ICSI (Kolettis and Thomas, 1997; Schlegel, 1997). Thus, the continued full evaluation and treatment of the male partner remains an important part of fertility treatment for the couple.</p><p>IVF and its variations have revolutionized the field of reproductive medicine during the past 25 years in ways that could not have been foreseen. This is particularly true for the treatment of the infertile male. Prior to the advent of IVF, severe male factor infertility had very limited and largely unsuccessful treatment options, and infertile couples either used donor sperm or adopted. In its initial years, IVF permitted fertilization attempts by severe oligo-, terato-, and/or asthenozoospermic males, although their success in fertilizing the ovum in vitro was markedly lower than that of the normospermic male. However, the introduction of ICSI in the 1990s allowed successful fertilization by a single isolated, immotile, and even, in some cases, dead sperm (Van Steirteghem et al, 1996). The combination of ICSI with TESE created treatment options for men whose ejaculate was azoospermic due to obstructive or nonobstructive causes, including those patients in whom only isolated pockets of spermatogenesis existed within the testes (Silber et al, 1995). Subsequent advances in this treatment modality include the cryopreservation of TESE sperm, which permits the advanced removal and storage of sperm prior to initiating an IVF cycle (Prins et al, 1999; Habermann et al, 2000). In 1980, Dr Alexander predicted that the use of testicular biopsy would decline, since it did not provide useful treatment options. It is noteworthy, however, that Dr Alexander predicted a renewed interest in testicular biopsies if biochemical and metabolic studies led to effective treatments for pathologic conditions that were previously unrecognized or untreatable. This prediction has been partially realized— however, it was through TESE-ICSI rather than biochemical methods. In fact, testicular biopsy can be combined with TESE—sperm cryopreservation both to diagnose and treat infertility in a single procedure (Schoor et al, 2002), and this approach is now used in many centers worldwide.</p><p>When the first IVF baby was born 25 years ago, the common practice for treating the infertile couple was artificial insemination using either the partner's sperm (AI-partner) or donor sperm (TDI). AI-partner then became the first line of therapy prior to the more expensive ART approaches but, in recent years, has been used less as practitioners realized the greater effectiveness of ART in treating male factor infertility. The epidemic of HIV that began in the 1980s radically changed the practice of sperm donor screening and use. Today, all TDI procedures use sperm that was frozen and stored in liquid nitrogen “quarantine” while the donor was extensively screened for genetic abnormalities and infectious agents. This practice led to needed improvements in the cryopreservation approaches for human sperm that Dr Alexander had requested in 1980. The improvements in freeze-thaw outcomes are due, in part, to the development of complex semen extenders and buffer systems that are now commercially available (Weidel and Prins, 1987). However, we still lack and need a testing modality that will predict the freezing success and subsequent fertilizing potential of frozen-thawed human sperm prior to the commencement of sperm freezing.</p><p>Dr Alexander called for an increased focus on the interaction of the male reproductive system with other body systems—“the organism as a whole.” What insight she had. In the past few years, the field of Men's Health has emerged as a new health emphasis area. In fact, this topic was the theme of the 2004 ASA postgraduate course titled “Men's Health: On the Horizons of Andrology.” Renowned experts presented lectures on androgen physiology in men, cardiovascular repercussions, sexual and psychosocial health, osteoporosis in men, use and abuse of anabolic steroids in sports, and trans-sexualism to provide a framework and vision to facilitate future contributions by andrologists to these important areas. The ASA shares its commitment to this endeavor with many organizations, including the NIH, in recognizing Men's Health as an important issue for the 20th century. Dr Alexander's vision and hope for a holistic approach to andrology is finally being realized.</p><p>From time to time, it is useful for a profession to review its history and take stock of its progress and obstacles. We are fortunate that our past President Dr Alexander provided the ASA with a blueprint for the future that now becomes a lens to focus on our past accomplishments and failures. We challenge one or several of our members to replicate her audacious insights with predictions for the next quarter century.</p>","PeriodicalId":15029,"journal":{"name":"Journal of andrology","volume":"25 4","pages":"435-440"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/j.1939-4640.2004.tb02812.x","citationCount":"6","resultStr":"{\"title\":\"The 25th Volume: President's Message: Andrology in the 20th Century: A Commentary on Our Progress During the Past 25 Years\",\"authors\":\"Gail S. Prins, William Bremner\",\"doi\":\"10.1002/j.1939-4640.2004.tb02812.x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In a heartbeat, we are there. Twenty-five years ago, Dr Nancy Alexander, President of the American Society of Andrology (ASA), delivered a Presidential Address at the 1980 ASA Annual Meeting in Chicago where she shared with us her perceptions for the future of andrology by the year 2000. This “state-of-the-art” address, titled “Andrology in the Year 2000,” was published in its entirety in the first volume of the <i>Journal of Andrology</i> (<i>J Androl</i>. 1980;1:149–157). It's a wonderful set of predictions, and we encourage our readers to go back to this manuscript and read (or reread) her insightful comments made at a time when the field of andrology was relatively new. The focus of Dr Alexander's comments and predictions for the year 2000 was not the entire field of andrology, but rather, 2 facets that are her area of expertise: 1) advances in male contraception, and 2) basic and clinical studies on development and maintenance of male fertility. In celebration of the Silver Anniversary of the <i>Journal of Andrology</i>, the 2004 ASA Presidents now reflect on Dr Alexander's comments and describe how the subsequent events during the past 25 years have confirmed or changed her predictions for andrology in the year 2000.</p><p>In 1978, National Institutes of Health (NIH) funding for population research had grown considerably from the previous 15 years and reached a total of $112 million set aside for the year. The ratio of male-female reproductive system funding was approximately 1:2, which was a vast improvement over the 1:4 ratio in 1972 (Alexander, 1980). The future for male reproductive research was promising. To address the current status of NIH funding for reproductive research, we asked the National Institute of Child Health and Human Development (NICHD) of the NIH to provide data on their funding levels during the past 5 years (1999–2003) in the areas of male and female reproductive research. It is important to stress that these numbers reflect NICHD funding only and do not include male reproductive system research by other institutes such as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the National Institute on Aging (NIA), and the National Institute of Environmental Health Sciences (NIEHS), all of which have research programs that include the male reproductive tract. Nonetheless, the NICHD is considered the primary institute for reproductive research and can be used as an indicator of fiscal commitments to reproductive research. Three categories were defined for analysis and are shown in the Figure: 1) targeted male reproductive health (research that applies only to male reproductive health [eg, endocrine regulation of germ cell apoptosis in the male, examinations of male fertility, Sertoli cell development]), 2) targeted female reproductive health (research that applies only to female reproductive health [eg, gonadotropin secretion during lactation, progestin regulation of uterine hemostasis and angiogenesis, prevalence and etiologic predictors of vulvodynia]), and 3) research applicable to both male and female reproductive health and not included in categories 1 or 2 (eg, sperm—egg interactions, human immunodeficiency virus [HIV] prevention methods, efficacy of infertility treatments). Data collected for these 3 categories between 1992 and 1998 indicated a steady funding level at a 1:2 ratio for male-female targeted research, as it was in 1978. With the concerted effort to double the NIH budget between 1998 and 2002, there was a marked increase in research funding in all 3 categories (Figure). That's the good (great) news. The bad news is that funding increases in male reproductive health research lagged behind those for female (category 2) and male and female (category 3) reproductive health research, bringing the simplistic male-female research ratio close to 1:4 again, the value in 1972. Explanations for the disparate funding increases are multifactorial and include the initiation of the Women's Reproductive Health Research career development programs and the NICHD's collaboration with the Office of Women's Health to administer the “Building Interdisciplinary Research in Women's Health.” Nonetheless, it is disheartening to see a return to greater disparity between male and female reproductive health emphasis at the NICHD rather than the reduced disparity predicted by Dr Alexander 25 years ago. Several key factors also contributed to the increased level of funding for research that is applicable to both male and female reproductive health during the past 5 years. For instance, the NICHD is now supporting the development and operation of a Biological Testing Facility and a Peptide Synthesis Facility. These facilities help researchers develop and assess the potential clinical uses of new compounds and formulations. Another contributing factor is that the NICHD has taken the opportunity to fund research under Center Core Grants that the National Institute of Allergy and Infectious Diseases manages. All of these activities include research applicable to male reproductive health, so there is optimism in these numbers as well. We hope that the expected downturn in NIH funding levels during the next several years will not too negatively affect the field of andrology.</p><p>Dr Alexander mentioned several aspects of the hormonal control of human spermatogenesis and the initial approaches to contraception using endocrine (steroid) administration. She predicted that by 2000, we would not have a male pill but that potential products would be undergoing testing. Both of these predictions have proven correct. However, she predicted that the approaches being tested in the early years of the new millennium would not be steroids. This prediction was not correct; all the major trials in recent years have involved steroids, particularly regimens combining an androgen (various forms of testosterone) and progestins (such as desogestrel, levonorgestrel, depot medroxyprogesterone acetate, norethisterone enanthate). Such regimens are now quite effective; the pharmaceutical industry (at least in Europe) has taken notice, and a multicenter trial, sponsored by Organon and Schering, is under way using testosterone undecanoate and 3-keto desogestrel. Unfortunately, the planned participation by 2 US centers in this study was prevented by the Food and Drug Administration, which is requiring additional animal data. Dr Alexander suggested that superactive analogs of gonadotropin-releasing hormone (GnRH) combined with testosterone would provide adequate spermatogenic suppression. This approach has been disappointing, but the possible utility of antagonist analogs of GnRH, particularly in induction regimens, is under active investigation in combination regimens with various testosterone compounds and formulations.</p><p>The prediction of Dr Alexander that, by 2000, we would be closer to an immunologic method of preventing male fertility has not proven to be correct. These approaches have foundered on difficulties with reliable induction of fertility suppression, unpredictable return to fertility, and adverse side effects. No such technique is in clinical trials, nor are animal studies particularly promising. Substantially greater understanding of the basic control mechanisms of immunology will be required prior to readdressing the clinical application of immunologic approaches.</p><p>Finally, Dr Alexander's own findings of increased atherosclerotic disease following vasectomy in animals have not been confirmed in extensive studies of men. Therefore, her prediction that this putative complication would decrease the numbers of vasectomies has not been borne out by subsequent clinical experience. Vasectomy remains a very effective, safe, and widely used method for permanent fertility control in men.</p><p>Extensive research on the epididymis has been conducted during the past quarter century, and several of the issues addressed by Dr Alexander with regard to epididymal function, protein secretions, and histology are beginning to be unraveled. For example, one set of experiments has shown the importance of the initial segment, at least in mice. Knockouts of the orphan tyrosine kinase receptor c-Ros show an undeveloped initial segment and male infertility (Sonnenberg-Riethmacher et al, 1996). The infertility defect appears to be due to a defect in tail angulation, and thus, the sperm fail to reach the egg. Tantalizing evidence suggests that the infertility phenotype is due to the failure of sperm to regulate their cell volume, which may be due to an altered epididymal luminal fluid microenvironment (Yeung et al, 2000). In 1980, although a few components of epididymal secretions had been identified, we had no idea about their role in sperm maturation, their maintenance during storage, or their activity after ejaculation. Scientists now have some evidence-based ideas. One current hypothesis is that organic solutes secreted into the epididymal lumen are osmolytes that regulate water movement into and out of both sperm and epididymal epithelial cells, similar to their role in the kidney. That solutes such as inositol, <span>l</span>-carnitine, glycerophosphorylcholine, and glutamate are found in the 50–60 mmol/L range (Hinton and Palladino, 1995) lends support for this role. Furthermore, osmolytes may protect sperm cells from rapid changes in osmolarity, which is important, since epididymal luminal fluid is hyperosmotic.</p><p>In 1980, Dr Alexander stated that “Only initial studies have been done on the various protein components… of the epididymal secretions” and predicted that their identification would eventually lead to new treatment methods for infertility. Following the revolution in molecular biology, this is currently the most studied aspect of epididymal biology, and many proteins have been recently discovered. While some proteins are unique to the epididymis, others are ubiquitous. The challenge to uncover their role(s) remains, since only a few secreted proteins have been assigned some kind of function. For example, the epididymis secretes defensins and defensin-like molecules, presumably for the protection of sperm and the epididymis itself (Von Horsten et al, 2002; Rao et al, 2003). CRISP-1 is a secreted protein that may be involved in either capacitation or sperm—egg binding (Cohen et al, 2000; Roberts et al, 2003). Other proteins have been identified with a putative function (eg, proteases, protease inhibitors, other enzymes), but again, their role in sperm maturation (if indeed there is one) is unknown. One recent leap forward is the identification of transporters in both sperm and epididymal epithelial cells, which has helped researchers understand how the epididymis forms the specialized luminal fluid environment. For example, several water, ion, and organic solute transporters have been identified and include the aquaporins; hydrogen plus adenosine triphosphatase for hydrogen ion transport; NHE-RF, a transporter involved in sodium/bicarbonate transport; and OCTN2, which transports <span>l</span>-carnitine (Breton et al, 1998; Bagnis et al, 2001; Rodriguez et al, 2002; Cheung et al, 2003). It is likely that no single secretory component is responsible for sperm maturation, but rather, that this process involves a complex series or cascade of events involving multiple cell—cell interactions.</p><p>A call was made for the development of research tools for the localization of cellular components. Considerable advances have been made in this field, and more and more proteins have been localized in different epididymal cell types. With laser capture technology, it is now possible to capture individual epithelial cells and perform reverse transcriptase-polymerase chain reaction (Kirby et al, 2003), generate complementary DNA libraries, and perform gene arrays. Hence, it is predicted that, in a few years, we will have a more thorough idea of the function of each epididymal cell type. Nonetheless, we still lack an understanding of the fundamental cell biology of epididymal function—protein synthesis, trafficking, secretion, and endocytosis, for instance, and this remains an area of future need. With advances in imaging, we can now perform in situ hybridization with immunohistochemistry, observe calcium movements in real time, and track epididymal development and fluid movement with time-lapse microscopy; thus, further advances are on the horizon. With more gene promoters being analyzed, it will not be too long before it will be possible to target gene silencing agents to specific epididymal cell types, as is already done to some regions of the epididymis. Hence, these approaches may also provide valuable information on the function of some genes/proteins in a cell type in a particular epididymal region in the very near future.</p><p>Major advances were made during the past quarter century to standardize semen analysis within the andrology community. Andrology laboratories in the United States now are included under the Clinical Laboratory Improvement Act (CLIA), which considers semen analysis a high-complexity test. Among other regulations, this designation requires adherence to strict standards, including daily quality control, laboratory certification or accreditation with attendant inspections, and oversight of a board-certified, doctoral-level laboratory director. Consequently, proficiency testing is now available from many providers for sperm concentration, viability, morphology, antisperm antibody assessment, and, most recently, motility. This semiannual assessment demonstrates a laboratory's ability to accurately analyze these male reproductive measures. Changes to CLIA now include periodic technologist competency testing, which is commercially available.</p><p>The World Health Organization (WHO) <i>Laboratory Manual for the Examination of Human Semen</i> is now published in its 4th edition and, since 1980, has set performance and evaluation recommendations that are used worldwide (WHO, 1999). Although semen analysis standards were not published by the ASA as Dr Alexander thought appropriate, many current and past ASA members have been intimately involved in writing these and other guidelines with the worldwide community. That we are now working from the 4th edition speaks for the fact that semen analysis, like all laboratory testing, requires continuous updating and reevaluation. This is most apparent in the area of sperm morphology, where evaluation systems have changed markedly over the years. In fact, this past year at the 2004 ASA Annual Meeting, a full-day Sperm Morphology Workshop was held that focused on laboratory-based training of the 2 most popular sperm morphology classification systems used by fertility specialists today: the WHO 3rd edition and the WHO 4th edition, also known as Strict Criteria. Unfortunately, clear standards for these systems are lacking, making the reproducibility of analysis difficult. We continue to need consistency and training for the clinical laboratory as well as for toxicology and industrial studies, which are now mandated in the United States.</p><p>During the past 20 years, we witnessed the introduction and use of computer-assisted semen analysis (CASA) systems for sperm concentration and motility analysis in the clinical and research andrology laboratory. While broadening and quantifying our information on motility parameters, these CASA systems, when used correctly, can reduce subjective variability in semen analysis across technicians in a single laboratory and even between laboratories. However, useful clinical correlates for all of the new motility information are still lacking and remain an area of future research. The application of CASA to morphometric analysis of sperm is relatively new, and its use is hampered by a lack of clear morphology standards. The cost and complexity of most CASA instruments remain significant barriers to their widespread adoption.</p><p>The past 25 years have brought enormous advances and uses for andrology testing and application above and beyond what was anticipated by Dr Alexander or anyone else, for that matter. The Hamster Ova—Sperm Penetration Assay or SPA, introduced by Rogers (1985), became a standard tool for the comprehensive andrology laboratory as predicted. Throughout the 1980s and 1990s, the SPA was widely used for evaluating the fertilizing potential of human spermatozoa with a discriminating power greater than that of the semen analysis alone (Rogers, 1985). As predicted, this technology was marketed by several commercial ventures. Reference laboratories developed systems for overnight transportation of sperm samples, which allowed centralized laboratories to perform the SPA for clinicians across the country and made this test widely available. Additionally, several companies sold frozen hamster ova, which made offering this assay a possibility in andrology laboratories that did not have prior access to an animal facility. As in vitro fertilization (IVF) became common practice for achieving pregnancy in the infertile couple, the SPA proved to be predictive of fertilization success in vitro. However, with the advent of intracytoplasmic sperm injection (ICSI), the use of the SPA has waned considerably. Although this test was shown to be predicative of the need for ICSI (Gvakharia et al, 2000), the success of ICSI and its subsequent widespread use and application in almost every IVF clinic have rendered the labor-intensive and costly SPA obsolete.</p><p>It was predicted that cervical mucus penetration assays would become a routine andrology laboratory test and, indeed, this came to pass. This aided the physician in making choices for the use of artificial insemination or even sperm donor insemination when “hostile” mucus was encountered for the sperm from a female's partner. Antisperm antibody testing not only became standard in the andrology work-up but also highly specific with the introduction of the Immunobead Test, which identified the immunoglobulin subtype present on sperm or within the female genital tract (Carson et al, 1988). However, once again, with the commonplace use of IVF-ICSI for establishing pregnancies in the infertile couple, the use of both of these assays has waned considerably from their peak usage in the 1990s.</p><p>Newer andrology laboratory tests have been introduced during the past decade and, although not commonplace in the standard andrology laboratory, their availability in centralized reference laboratories has allowed their implementation when clinically necessary. The Sperm Chromatin Structure Assay assesses sperm DNA fragmentation and has been found to correlate with fertility potential (Evenson and Jost, 2000). In addition to its routine prognostic value, this cytometry assay is useful for evaluating men at increased risk for DNA damage that can follow occupational exposures, that can occur with aging, or that can follow freeze-thaw procedures. Discoveries in the field of genetics have led to Y-chromosome deletion testing for infertile men, and commercial kits are available for this purpose. Full deletions or microdeletions in the long arm of the Y chromosome (azoospermic factor or AZF regions) have been shown to cause azoospermia, oligozoospermia, and related male infertility problems, and the ability to screen for these in the infertile patient has vastly improved diagnostic capabilities (Kent-First et al, 1996; Reijo et al, 1996). The use of testicular sperm extraction (TESE) from azoospermic men, combined with IVF-ICSI to achieve fertilization, permits the transmission of Y-related infertility to the male offspring, making this testing modality imperative for informed decision making by the patients who undergo these procedures.</p><p>The past 25 years have seen the rise, as well as the subsequent decline, of intensive andrology testing in the work-up of the infertile couple. The ease and availability of assisted reproductive technologies (ART) have led many clinicians to implement these techniques quickly and to forgo a full diagnostic male evaluation. Although this approach may lead to a pregnancy in the short term, it carries the risk that the cause of infertility will go undiagnosed. Since infertility can be a marker of serious medical problems or toxicant exposures, denying the male partner a full work-up has important health consequences. Furthermore, several studies have shown that the cost-effectiveness (cost per live delivery) of treating more common male factor problems such as varicocele or vasal and/or epididymal obstruction is much greater than the initial use of IVF-ICSI (Kolettis and Thomas, 1997; Schlegel, 1997). Thus, the continued full evaluation and treatment of the male partner remains an important part of fertility treatment for the couple.</p><p>IVF and its variations have revolutionized the field of reproductive medicine during the past 25 years in ways that could not have been foreseen. This is particularly true for the treatment of the infertile male. Prior to the advent of IVF, severe male factor infertility had very limited and largely unsuccessful treatment options, and infertile couples either used donor sperm or adopted. In its initial years, IVF permitted fertilization attempts by severe oligo-, terato-, and/or asthenozoospermic males, although their success in fertilizing the ovum in vitro was markedly lower than that of the normospermic male. However, the introduction of ICSI in the 1990s allowed successful fertilization by a single isolated, immotile, and even, in some cases, dead sperm (Van Steirteghem et al, 1996). The combination of ICSI with TESE created treatment options for men whose ejaculate was azoospermic due to obstructive or nonobstructive causes, including those patients in whom only isolated pockets of spermatogenesis existed within the testes (Silber et al, 1995). Subsequent advances in this treatment modality include the cryopreservation of TESE sperm, which permits the advanced removal and storage of sperm prior to initiating an IVF cycle (Prins et al, 1999; Habermann et al, 2000). In 1980, Dr Alexander predicted that the use of testicular biopsy would decline, since it did not provide useful treatment options. It is noteworthy, however, that Dr Alexander predicted a renewed interest in testicular biopsies if biochemical and metabolic studies led to effective treatments for pathologic conditions that were previously unrecognized or untreatable. This prediction has been partially realized— however, it was through TESE-ICSI rather than biochemical methods. In fact, testicular biopsy can be combined with TESE—sperm cryopreservation both to diagnose and treat infertility in a single procedure (Schoor et al, 2002), and this approach is now used in many centers worldwide.</p><p>When the first IVF baby was born 25 years ago, the common practice for treating the infertile couple was artificial insemination using either the partner's sperm (AI-partner) or donor sperm (TDI). AI-partner then became the first line of therapy prior to the more expensive ART approaches but, in recent years, has been used less as practitioners realized the greater effectiveness of ART in treating male factor infertility. The epidemic of HIV that began in the 1980s radically changed the practice of sperm donor screening and use. Today, all TDI procedures use sperm that was frozen and stored in liquid nitrogen “quarantine” while the donor was extensively screened for genetic abnormalities and infectious agents. This practice led to needed improvements in the cryopreservation approaches for human sperm that Dr Alexander had requested in 1980. The improvements in freeze-thaw outcomes are due, in part, to the development of complex semen extenders and buffer systems that are now commercially available (Weidel and Prins, 1987). However, we still lack and need a testing modality that will predict the freezing success and subsequent fertilizing potential of frozen-thawed human sperm prior to the commencement of sperm freezing.</p><p>Dr Alexander called for an increased focus on the interaction of the male reproductive system with other body systems—“the organism as a whole.” What insight she had. In the past few years, the field of Men's Health has emerged as a new health emphasis area. In fact, this topic was the theme of the 2004 ASA postgraduate course titled “Men's Health: On the Horizons of Andrology.” Renowned experts presented lectures on androgen physiology in men, cardiovascular repercussions, sexual and psychosocial health, osteoporosis in men, use and abuse of anabolic steroids in sports, and trans-sexualism to provide a framework and vision to facilitate future contributions by andrologists to these important areas. The ASA shares its commitment to this endeavor with many organizations, including the NIH, in recognizing Men's Health as an important issue for the 20th century. Dr Alexander's vision and hope for a holistic approach to andrology is finally being realized.</p><p>From time to time, it is useful for a profession to review its history and take stock of its progress and obstacles. We are fortunate that our past President Dr Alexander provided the ASA with a blueprint for the future that now becomes a lens to focus on our past accomplishments and failures. We challenge one or several of our members to replicate her audacious insights with predictions for the next quarter century.</p>\",\"PeriodicalId\":15029,\"journal\":{\"name\":\"Journal of andrology\",\"volume\":\"25 4\",\"pages\":\"435-440\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/j.1939-4640.2004.tb02812.x\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of andrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/j.1939-4640.2004.tb02812.x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of andrology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/j.1939-4640.2004.tb02812.x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
摘要
随着分子生物学的革命,这是目前研究最多的附睾生物学方面,最近发现了许多蛋白质。虽然有些蛋白质是附睾特有的,但其他蛋白质是普遍存在的。发现它们的作用仍然是一个挑战,因为只有少数分泌的蛋白质被赋予了某种功能。例如,附睾分泌防御素和类似防御素的分子,可能是为了保护精子和附睾本身(Von Horsten et al ., 2002;Rao et al ., 2003)。CRISP-1是一种分泌蛋白,可能参与获能或精子-卵子结合(Cohen et al ., 2000;Roberts et al, 2003)。其他蛋白质已被确定具有假定的功能(例如,蛋白酶,蛋白酶抑制剂,其他酶),但它们在精子成熟中的作用(如果确实存在的话)仍是未知的。最近的一个飞跃是精子和附睾上皮细胞中转运蛋白的鉴定,这有助于研究人员了解附睾是如何形成专门的腔液环境的。例如,已经确定了几种水、离子和有机溶质转运体,包括水通道蛋白;氢离子运输的氢加腺苷三磷酸酶;NHE-RF,一种参与钠/碳酸氢盐运输的转运体;OCTN2,转运左旋肉碱(Breton等人,1998;Bagnis et al, 2001;Rodriguez et al, 2002;bbb10等人,2003)。很可能没有单一的分泌成分负责精子成熟,而是这个过程涉及一系列复杂的事件,涉及多个细胞-细胞相互作用。呼吁开发定位细胞成分的研究工具。这一领域已经取得了相当大的进展,越来越多的蛋白质被定位于不同类型的附睾细胞。利用激光捕获技术,现在可以捕获单个上皮细胞并进行逆转录-聚合酶链反应(Kirby等,2003),生成互补DNA文库,并进行基因阵列。因此,预计在几年内,我们将对每种附睾细胞类型的功能有更全面的了解。尽管如此,我们仍然缺乏对附睾功能的基本细胞生物学的理解-例如蛋白质合成,运输,分泌和内吞作用,这仍然是未来需要的领域。随着成像技术的进步,我们现在可以用免疫组织化学进行原位杂交,实时观察钙的运动,用延时显微镜跟踪附睾的发育和液体的运动;因此,进一步的进展即将出现。随着更多的基因启动子被分析,用不了多久,基因沉默剂就有可能针对特定的附睾细胞类型,就像已经对附睾的某些区域所做的那样。因此,在不久的将来,这些方法也可能为在特定附睾区域的细胞类型中某些基因/蛋白质的功能提供有价值的信息。在过去的25年里,男科学界在精液分析标准化方面取得了重大进展。美国的男科实验室现在被纳入临床实验室改进法案(CLIA),该法案认为精液分析是一项高度复杂的测试。在其他规定中,这一指定要求遵守严格的标准,包括日常质量控制,实验室认证或伴随检查的认可,以及董事会认证的博士级实验室主任的监督。因此,现在可以从许多精子浓度、活力、形态、抗精子抗体评估以及最近的能动性等方面进行熟练测试。这项半年一次的评估显示了实验室准确分析这些男性生殖指标的能力。CLIA的变化现在包括定期的技术人员能力测试,这是可商用的。世界卫生组织(世卫组织)《人类精液检查实验室手册》现已出版第四版,自1980年以来制定了在全世界使用的绩效和评价建议(世卫组织,1999年)。虽然精液分析标准没有像亚历山大博士认为的那样由ASA发布,但许多现任和过去的ASA成员一直密切参与编写这些指南和其他国际社会的指南。我们现在从第四版开始工作说明了一个事实,即精液分析,像所有实验室测试一样,需要不断更新和重新评估。这在精子形态学领域最为明显,多年来评估系统发生了显著变化。 事实上,在过去一年的2004年美国精子标准协会年会上,举办了一个全天的精子形态研讨会,重点是对当今生育专家使用的两种最流行的精子形态分类系统进行实验室培训:世卫组织第三版和世卫组织第四版,也称为严格标准。不幸的是,这些系统缺乏明确的标准,使得分析的再现性变得困难。我们继续需要临床实验室以及毒理学和工业研究的一致性和培训,这些现在在美国是强制性的。在过去的20年里,我们见证了计算机辅助精液分析(CASA)系统在临床和研究男科实验室中用于精子浓度和活力分析的引入和使用。在扩大和量化我们关于运动参数的信息的同时,这些CASA系统如果使用得当,可以减少单个实验室甚至实验室之间技术人员精液分析的主观差异。然而,对于所有新的运动信息的有用的临床相关性仍然缺乏,并且仍然是未来研究的领域。CASA在精子形态计量学分析中的应用相对较新,其应用受到缺乏明确形态学标准的阻碍。大多数CASA工具的成本和复杂性仍然是其广泛采用的重大障碍。在过去的25年里,男科测试和应用取得了巨大的进步,远远超出了亚历山大博士或其他任何人的预期。Rogers(1985)引入的仓鼠卵细胞-精子穿透试验(SPA),如预期的那样,成为综合男科实验室的标准工具。在整个20世纪80年代和90年代,SPA被广泛用于评估人类精子的受精潜力,其辨别能力比单独的精液分析更强(Rogers, 1985)。正如所预测的那样,这项技术已由几家商业企业推向市场。参考实验室开发了精子样本夜间运输系统,这使得集中实验室能够为全国各地的临床医生执行SPA,并使这项测试得到广泛应用。此外,几家公司出售冷冻仓鼠卵子,这使得在没有事先进入动物设施的男科实验室提供这种检测成为可能。随着体外受精(IVF)成为不育夫妇实现怀孕的常见做法,SPA被证明是体外受精成功的预测指标。然而,随着胞浆内单精子注射(ICSI)的出现,SPA的使用已经大大减少。虽然这项测试被证明是对ICSI需求的预测(Gvakharia等人,2000),但ICSI的成功及其随后在几乎每个IVF诊所的广泛使用和应用使得劳动密集型和昂贵的SPA过时了。据预测,宫颈黏液渗透试验将成为一项常规的男科实验室检查,事实也确实如此。这有助于医生在遇到来自女性伴侣的精子的“敌对”粘液时选择使用人工授精,甚至是精子供体授精。抗精子抗体检测不仅成为男科检查的标准,而且随着免疫珠试验的引入,抗精子抗体检测也变得高度特异性,免疫珠试验可识别存在于精子或女性生殖道内的免疫球蛋白亚型(Carson et al, 1988)。然而,再一次,随着IVF-ICSI在不育夫妇中建立怀孕的普遍使用,这两种检测方法的使用都从20世纪90年代的高峰使用大大减少。在过去的十年中,新的男科实验室测试已经被引入,尽管在标准男科实验室中并不常见,但在集中参考实验室中,它们的可用性允许在临床需要时实施。精子染色质结构分析评估精子DNA片段,并发现其与生育潜力相关(Evenson和Jost, 2000)。除了其常规预后价值外,这种细胞测定法还可用于评估职业暴露、衰老或冻融过程中DNA损伤风险增加的男性。遗传学领域的发现导致了对不育男性进行y染色体缺失测试,商业工具包可用于此目的。Y染色体长臂的完全缺失或微缺失(无精子因子或AZF区域)已被证明会导致无精子症、少精子症和相关的男性不育问题,在不育患者中筛查这些疾病的能力大大提高了诊断能力(Kent-First等人,1996;Reijo et al, 1996)。
The 25th Volume: President's Message: Andrology in the 20th Century: A Commentary on Our Progress During the Past 25 Years
In a heartbeat, we are there. Twenty-five years ago, Dr Nancy Alexander, President of the American Society of Andrology (ASA), delivered a Presidential Address at the 1980 ASA Annual Meeting in Chicago where she shared with us her perceptions for the future of andrology by the year 2000. This “state-of-the-art” address, titled “Andrology in the Year 2000,” was published in its entirety in the first volume of the Journal of Andrology (J Androl. 1980;1:149–157). It's a wonderful set of predictions, and we encourage our readers to go back to this manuscript and read (or reread) her insightful comments made at a time when the field of andrology was relatively new. The focus of Dr Alexander's comments and predictions for the year 2000 was not the entire field of andrology, but rather, 2 facets that are her area of expertise: 1) advances in male contraception, and 2) basic and clinical studies on development and maintenance of male fertility. In celebration of the Silver Anniversary of the Journal of Andrology, the 2004 ASA Presidents now reflect on Dr Alexander's comments and describe how the subsequent events during the past 25 years have confirmed or changed her predictions for andrology in the year 2000.
In 1978, National Institutes of Health (NIH) funding for population research had grown considerably from the previous 15 years and reached a total of $112 million set aside for the year. The ratio of male-female reproductive system funding was approximately 1:2, which was a vast improvement over the 1:4 ratio in 1972 (Alexander, 1980). The future for male reproductive research was promising. To address the current status of NIH funding for reproductive research, we asked the National Institute of Child Health and Human Development (NICHD) of the NIH to provide data on their funding levels during the past 5 years (1999–2003) in the areas of male and female reproductive research. It is important to stress that these numbers reflect NICHD funding only and do not include male reproductive system research by other institutes such as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the National Institute on Aging (NIA), and the National Institute of Environmental Health Sciences (NIEHS), all of which have research programs that include the male reproductive tract. Nonetheless, the NICHD is considered the primary institute for reproductive research and can be used as an indicator of fiscal commitments to reproductive research. Three categories were defined for analysis and are shown in the Figure: 1) targeted male reproductive health (research that applies only to male reproductive health [eg, endocrine regulation of germ cell apoptosis in the male, examinations of male fertility, Sertoli cell development]), 2) targeted female reproductive health (research that applies only to female reproductive health [eg, gonadotropin secretion during lactation, progestin regulation of uterine hemostasis and angiogenesis, prevalence and etiologic predictors of vulvodynia]), and 3) research applicable to both male and female reproductive health and not included in categories 1 or 2 (eg, sperm—egg interactions, human immunodeficiency virus [HIV] prevention methods, efficacy of infertility treatments). Data collected for these 3 categories between 1992 and 1998 indicated a steady funding level at a 1:2 ratio for male-female targeted research, as it was in 1978. With the concerted effort to double the NIH budget between 1998 and 2002, there was a marked increase in research funding in all 3 categories (Figure). That's the good (great) news. The bad news is that funding increases in male reproductive health research lagged behind those for female (category 2) and male and female (category 3) reproductive health research, bringing the simplistic male-female research ratio close to 1:4 again, the value in 1972. Explanations for the disparate funding increases are multifactorial and include the initiation of the Women's Reproductive Health Research career development programs and the NICHD's collaboration with the Office of Women's Health to administer the “Building Interdisciplinary Research in Women's Health.” Nonetheless, it is disheartening to see a return to greater disparity between male and female reproductive health emphasis at the NICHD rather than the reduced disparity predicted by Dr Alexander 25 years ago. Several key factors also contributed to the increased level of funding for research that is applicable to both male and female reproductive health during the past 5 years. For instance, the NICHD is now supporting the development and operation of a Biological Testing Facility and a Peptide Synthesis Facility. These facilities help researchers develop and assess the potential clinical uses of new compounds and formulations. Another contributing factor is that the NICHD has taken the opportunity to fund research under Center Core Grants that the National Institute of Allergy and Infectious Diseases manages. All of these activities include research applicable to male reproductive health, so there is optimism in these numbers as well. We hope that the expected downturn in NIH funding levels during the next several years will not too negatively affect the field of andrology.
Dr Alexander mentioned several aspects of the hormonal control of human spermatogenesis and the initial approaches to contraception using endocrine (steroid) administration. She predicted that by 2000, we would not have a male pill but that potential products would be undergoing testing. Both of these predictions have proven correct. However, she predicted that the approaches being tested in the early years of the new millennium would not be steroids. This prediction was not correct; all the major trials in recent years have involved steroids, particularly regimens combining an androgen (various forms of testosterone) and progestins (such as desogestrel, levonorgestrel, depot medroxyprogesterone acetate, norethisterone enanthate). Such regimens are now quite effective; the pharmaceutical industry (at least in Europe) has taken notice, and a multicenter trial, sponsored by Organon and Schering, is under way using testosterone undecanoate and 3-keto desogestrel. Unfortunately, the planned participation by 2 US centers in this study was prevented by the Food and Drug Administration, which is requiring additional animal data. Dr Alexander suggested that superactive analogs of gonadotropin-releasing hormone (GnRH) combined with testosterone would provide adequate spermatogenic suppression. This approach has been disappointing, but the possible utility of antagonist analogs of GnRH, particularly in induction regimens, is under active investigation in combination regimens with various testosterone compounds and formulations.
The prediction of Dr Alexander that, by 2000, we would be closer to an immunologic method of preventing male fertility has not proven to be correct. These approaches have foundered on difficulties with reliable induction of fertility suppression, unpredictable return to fertility, and adverse side effects. No such technique is in clinical trials, nor are animal studies particularly promising. Substantially greater understanding of the basic control mechanisms of immunology will be required prior to readdressing the clinical application of immunologic approaches.
Finally, Dr Alexander's own findings of increased atherosclerotic disease following vasectomy in animals have not been confirmed in extensive studies of men. Therefore, her prediction that this putative complication would decrease the numbers of vasectomies has not been borne out by subsequent clinical experience. Vasectomy remains a very effective, safe, and widely used method for permanent fertility control in men.
Extensive research on the epididymis has been conducted during the past quarter century, and several of the issues addressed by Dr Alexander with regard to epididymal function, protein secretions, and histology are beginning to be unraveled. For example, one set of experiments has shown the importance of the initial segment, at least in mice. Knockouts of the orphan tyrosine kinase receptor c-Ros show an undeveloped initial segment and male infertility (Sonnenberg-Riethmacher et al, 1996). The infertility defect appears to be due to a defect in tail angulation, and thus, the sperm fail to reach the egg. Tantalizing evidence suggests that the infertility phenotype is due to the failure of sperm to regulate their cell volume, which may be due to an altered epididymal luminal fluid microenvironment (Yeung et al, 2000). In 1980, although a few components of epididymal secretions had been identified, we had no idea about their role in sperm maturation, their maintenance during storage, or their activity after ejaculation. Scientists now have some evidence-based ideas. One current hypothesis is that organic solutes secreted into the epididymal lumen are osmolytes that regulate water movement into and out of both sperm and epididymal epithelial cells, similar to their role in the kidney. That solutes such as inositol, l-carnitine, glycerophosphorylcholine, and glutamate are found in the 50–60 mmol/L range (Hinton and Palladino, 1995) lends support for this role. Furthermore, osmolytes may protect sperm cells from rapid changes in osmolarity, which is important, since epididymal luminal fluid is hyperosmotic.
In 1980, Dr Alexander stated that “Only initial studies have been done on the various protein components… of the epididymal secretions” and predicted that their identification would eventually lead to new treatment methods for infertility. Following the revolution in molecular biology, this is currently the most studied aspect of epididymal biology, and many proteins have been recently discovered. While some proteins are unique to the epididymis, others are ubiquitous. The challenge to uncover their role(s) remains, since only a few secreted proteins have been assigned some kind of function. For example, the epididymis secretes defensins and defensin-like molecules, presumably for the protection of sperm and the epididymis itself (Von Horsten et al, 2002; Rao et al, 2003). CRISP-1 is a secreted protein that may be involved in either capacitation or sperm—egg binding (Cohen et al, 2000; Roberts et al, 2003). Other proteins have been identified with a putative function (eg, proteases, protease inhibitors, other enzymes), but again, their role in sperm maturation (if indeed there is one) is unknown. One recent leap forward is the identification of transporters in both sperm and epididymal epithelial cells, which has helped researchers understand how the epididymis forms the specialized luminal fluid environment. For example, several water, ion, and organic solute transporters have been identified and include the aquaporins; hydrogen plus adenosine triphosphatase for hydrogen ion transport; NHE-RF, a transporter involved in sodium/bicarbonate transport; and OCTN2, which transports l-carnitine (Breton et al, 1998; Bagnis et al, 2001; Rodriguez et al, 2002; Cheung et al, 2003). It is likely that no single secretory component is responsible for sperm maturation, but rather, that this process involves a complex series or cascade of events involving multiple cell—cell interactions.
A call was made for the development of research tools for the localization of cellular components. Considerable advances have been made in this field, and more and more proteins have been localized in different epididymal cell types. With laser capture technology, it is now possible to capture individual epithelial cells and perform reverse transcriptase-polymerase chain reaction (Kirby et al, 2003), generate complementary DNA libraries, and perform gene arrays. Hence, it is predicted that, in a few years, we will have a more thorough idea of the function of each epididymal cell type. Nonetheless, we still lack an understanding of the fundamental cell biology of epididymal function—protein synthesis, trafficking, secretion, and endocytosis, for instance, and this remains an area of future need. With advances in imaging, we can now perform in situ hybridization with immunohistochemistry, observe calcium movements in real time, and track epididymal development and fluid movement with time-lapse microscopy; thus, further advances are on the horizon. With more gene promoters being analyzed, it will not be too long before it will be possible to target gene silencing agents to specific epididymal cell types, as is already done to some regions of the epididymis. Hence, these approaches may also provide valuable information on the function of some genes/proteins in a cell type in a particular epididymal region in the very near future.
Major advances were made during the past quarter century to standardize semen analysis within the andrology community. Andrology laboratories in the United States now are included under the Clinical Laboratory Improvement Act (CLIA), which considers semen analysis a high-complexity test. Among other regulations, this designation requires adherence to strict standards, including daily quality control, laboratory certification or accreditation with attendant inspections, and oversight of a board-certified, doctoral-level laboratory director. Consequently, proficiency testing is now available from many providers for sperm concentration, viability, morphology, antisperm antibody assessment, and, most recently, motility. This semiannual assessment demonstrates a laboratory's ability to accurately analyze these male reproductive measures. Changes to CLIA now include periodic technologist competency testing, which is commercially available.
The World Health Organization (WHO) Laboratory Manual for the Examination of Human Semen is now published in its 4th edition and, since 1980, has set performance and evaluation recommendations that are used worldwide (WHO, 1999). Although semen analysis standards were not published by the ASA as Dr Alexander thought appropriate, many current and past ASA members have been intimately involved in writing these and other guidelines with the worldwide community. That we are now working from the 4th edition speaks for the fact that semen analysis, like all laboratory testing, requires continuous updating and reevaluation. This is most apparent in the area of sperm morphology, where evaluation systems have changed markedly over the years. In fact, this past year at the 2004 ASA Annual Meeting, a full-day Sperm Morphology Workshop was held that focused on laboratory-based training of the 2 most popular sperm morphology classification systems used by fertility specialists today: the WHO 3rd edition and the WHO 4th edition, also known as Strict Criteria. Unfortunately, clear standards for these systems are lacking, making the reproducibility of analysis difficult. We continue to need consistency and training for the clinical laboratory as well as for toxicology and industrial studies, which are now mandated in the United States.
During the past 20 years, we witnessed the introduction and use of computer-assisted semen analysis (CASA) systems for sperm concentration and motility analysis in the clinical and research andrology laboratory. While broadening and quantifying our information on motility parameters, these CASA systems, when used correctly, can reduce subjective variability in semen analysis across technicians in a single laboratory and even between laboratories. However, useful clinical correlates for all of the new motility information are still lacking and remain an area of future research. The application of CASA to morphometric analysis of sperm is relatively new, and its use is hampered by a lack of clear morphology standards. The cost and complexity of most CASA instruments remain significant barriers to their widespread adoption.
The past 25 years have brought enormous advances and uses for andrology testing and application above and beyond what was anticipated by Dr Alexander or anyone else, for that matter. The Hamster Ova—Sperm Penetration Assay or SPA, introduced by Rogers (1985), became a standard tool for the comprehensive andrology laboratory as predicted. Throughout the 1980s and 1990s, the SPA was widely used for evaluating the fertilizing potential of human spermatozoa with a discriminating power greater than that of the semen analysis alone (Rogers, 1985). As predicted, this technology was marketed by several commercial ventures. Reference laboratories developed systems for overnight transportation of sperm samples, which allowed centralized laboratories to perform the SPA for clinicians across the country and made this test widely available. Additionally, several companies sold frozen hamster ova, which made offering this assay a possibility in andrology laboratories that did not have prior access to an animal facility. As in vitro fertilization (IVF) became common practice for achieving pregnancy in the infertile couple, the SPA proved to be predictive of fertilization success in vitro. However, with the advent of intracytoplasmic sperm injection (ICSI), the use of the SPA has waned considerably. Although this test was shown to be predicative of the need for ICSI (Gvakharia et al, 2000), the success of ICSI and its subsequent widespread use and application in almost every IVF clinic have rendered the labor-intensive and costly SPA obsolete.
It was predicted that cervical mucus penetration assays would become a routine andrology laboratory test and, indeed, this came to pass. This aided the physician in making choices for the use of artificial insemination or even sperm donor insemination when “hostile” mucus was encountered for the sperm from a female's partner. Antisperm antibody testing not only became standard in the andrology work-up but also highly specific with the introduction of the Immunobead Test, which identified the immunoglobulin subtype present on sperm or within the female genital tract (Carson et al, 1988). However, once again, with the commonplace use of IVF-ICSI for establishing pregnancies in the infertile couple, the use of both of these assays has waned considerably from their peak usage in the 1990s.
Newer andrology laboratory tests have been introduced during the past decade and, although not commonplace in the standard andrology laboratory, their availability in centralized reference laboratories has allowed their implementation when clinically necessary. The Sperm Chromatin Structure Assay assesses sperm DNA fragmentation and has been found to correlate with fertility potential (Evenson and Jost, 2000). In addition to its routine prognostic value, this cytometry assay is useful for evaluating men at increased risk for DNA damage that can follow occupational exposures, that can occur with aging, or that can follow freeze-thaw procedures. Discoveries in the field of genetics have led to Y-chromosome deletion testing for infertile men, and commercial kits are available for this purpose. Full deletions or microdeletions in the long arm of the Y chromosome (azoospermic factor or AZF regions) have been shown to cause azoospermia, oligozoospermia, and related male infertility problems, and the ability to screen for these in the infertile patient has vastly improved diagnostic capabilities (Kent-First et al, 1996; Reijo et al, 1996). The use of testicular sperm extraction (TESE) from azoospermic men, combined with IVF-ICSI to achieve fertilization, permits the transmission of Y-related infertility to the male offspring, making this testing modality imperative for informed decision making by the patients who undergo these procedures.
The past 25 years have seen the rise, as well as the subsequent decline, of intensive andrology testing in the work-up of the infertile couple. The ease and availability of assisted reproductive technologies (ART) have led many clinicians to implement these techniques quickly and to forgo a full diagnostic male evaluation. Although this approach may lead to a pregnancy in the short term, it carries the risk that the cause of infertility will go undiagnosed. Since infertility can be a marker of serious medical problems or toxicant exposures, denying the male partner a full work-up has important health consequences. Furthermore, several studies have shown that the cost-effectiveness (cost per live delivery) of treating more common male factor problems such as varicocele or vasal and/or epididymal obstruction is much greater than the initial use of IVF-ICSI (Kolettis and Thomas, 1997; Schlegel, 1997). Thus, the continued full evaluation and treatment of the male partner remains an important part of fertility treatment for the couple.
IVF and its variations have revolutionized the field of reproductive medicine during the past 25 years in ways that could not have been foreseen. This is particularly true for the treatment of the infertile male. Prior to the advent of IVF, severe male factor infertility had very limited and largely unsuccessful treatment options, and infertile couples either used donor sperm or adopted. In its initial years, IVF permitted fertilization attempts by severe oligo-, terato-, and/or asthenozoospermic males, although their success in fertilizing the ovum in vitro was markedly lower than that of the normospermic male. However, the introduction of ICSI in the 1990s allowed successful fertilization by a single isolated, immotile, and even, in some cases, dead sperm (Van Steirteghem et al, 1996). The combination of ICSI with TESE created treatment options for men whose ejaculate was azoospermic due to obstructive or nonobstructive causes, including those patients in whom only isolated pockets of spermatogenesis existed within the testes (Silber et al, 1995). Subsequent advances in this treatment modality include the cryopreservation of TESE sperm, which permits the advanced removal and storage of sperm prior to initiating an IVF cycle (Prins et al, 1999; Habermann et al, 2000). In 1980, Dr Alexander predicted that the use of testicular biopsy would decline, since it did not provide useful treatment options. It is noteworthy, however, that Dr Alexander predicted a renewed interest in testicular biopsies if biochemical and metabolic studies led to effective treatments for pathologic conditions that were previously unrecognized or untreatable. This prediction has been partially realized— however, it was through TESE-ICSI rather than biochemical methods. In fact, testicular biopsy can be combined with TESE—sperm cryopreservation both to diagnose and treat infertility in a single procedure (Schoor et al, 2002), and this approach is now used in many centers worldwide.
When the first IVF baby was born 25 years ago, the common practice for treating the infertile couple was artificial insemination using either the partner's sperm (AI-partner) or donor sperm (TDI). AI-partner then became the first line of therapy prior to the more expensive ART approaches but, in recent years, has been used less as practitioners realized the greater effectiveness of ART in treating male factor infertility. The epidemic of HIV that began in the 1980s radically changed the practice of sperm donor screening and use. Today, all TDI procedures use sperm that was frozen and stored in liquid nitrogen “quarantine” while the donor was extensively screened for genetic abnormalities and infectious agents. This practice led to needed improvements in the cryopreservation approaches for human sperm that Dr Alexander had requested in 1980. The improvements in freeze-thaw outcomes are due, in part, to the development of complex semen extenders and buffer systems that are now commercially available (Weidel and Prins, 1987). However, we still lack and need a testing modality that will predict the freezing success and subsequent fertilizing potential of frozen-thawed human sperm prior to the commencement of sperm freezing.
Dr Alexander called for an increased focus on the interaction of the male reproductive system with other body systems—“the organism as a whole.” What insight she had. In the past few years, the field of Men's Health has emerged as a new health emphasis area. In fact, this topic was the theme of the 2004 ASA postgraduate course titled “Men's Health: On the Horizons of Andrology.” Renowned experts presented lectures on androgen physiology in men, cardiovascular repercussions, sexual and psychosocial health, osteoporosis in men, use and abuse of anabolic steroids in sports, and trans-sexualism to provide a framework and vision to facilitate future contributions by andrologists to these important areas. The ASA shares its commitment to this endeavor with many organizations, including the NIH, in recognizing Men's Health as an important issue for the 20th century. Dr Alexander's vision and hope for a holistic approach to andrology is finally being realized.
From time to time, it is useful for a profession to review its history and take stock of its progress and obstacles. We are fortunate that our past President Dr Alexander provided the ASA with a blueprint for the future that now becomes a lens to focus on our past accomplishments and failures. We challenge one or several of our members to replicate her audacious insights with predictions for the next quarter century.
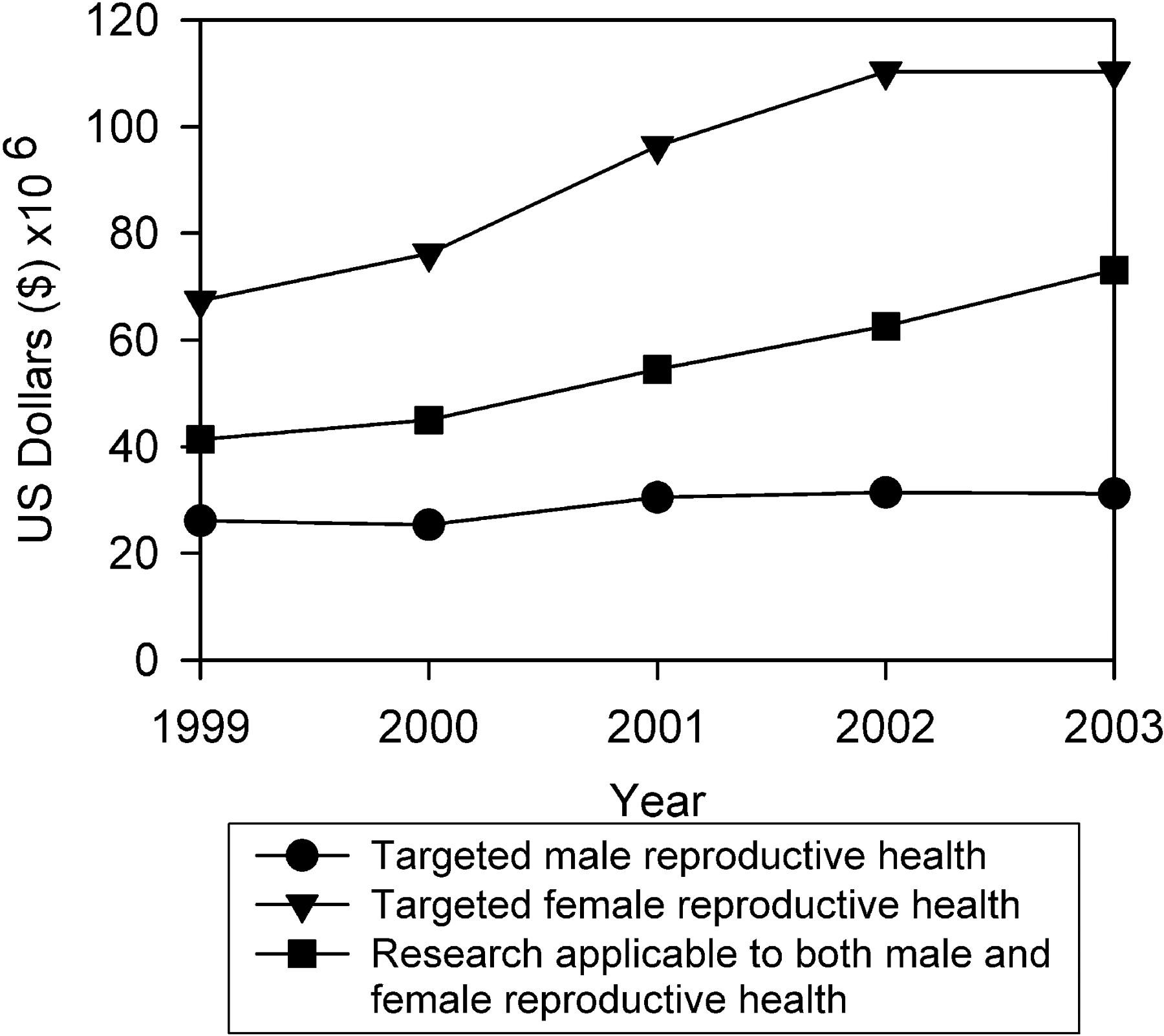

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


