{"title":"服用褪黑素会改变正常男性的精液质量","authors":"Alexander Lerchl, Rafael Luboshitzky","doi":"10.1002/j.1939-4640.2004.tb02778.x","DOIUrl":null,"url":null,"abstract":"<p><i>To the Editor</i>:</p><p>The publication by Luboshitzky et al (2002) concerning the effects of melatonin on human sperm quality deserves strong critique for a number of reasons. The authors performed a double-blind crossover study during which healthy volunteers were given either melatonin (3 mg) or a placebo for 3 months each, while between the phases, a washout phase of 2 weeks was included. At the beginning and end of the 2 phases, a total of 11 parameters (sperm and endocrine) were measured and, again, 3 and 6 months after the end of the study. According to the results (!!), volunteers were divided into 2 groups, responders (n = 2) and nonresponders (n = 6). The criterion was that both sperm concentration and sperm motility “dropped during the melatonin treatment period.” Both of these men belonged to the group to which melatonin was given in the second treatment period. The title and the conclusions of this paper are simply not justified by the data for the following reasons:</p><p>In summary, I see no evidence whatsoever for the conclusion that melatonin impairs sperm parameters in healthy men. It rather appears that an expected result influenced the way the data were handled.</p><p><i>To the Editor</i>:</p><p>We appreciate the comments of Lerchl (2004) regarding the effect of exogenous melatonin on sperm quality in normal men (Luboshitzky et al, 2002). In this study, we examined the possible effect of melatonin on semen concentration, motility, and morphology in 8 healthy young men. Since we did not study fertility in the general sense, we performed one semen analysis at baseline. We fully agree that 2 semen samples are indicated for the initial evaluation of fertility. In our study, we defined a subject as a responder if his sperm concentration and motility dropped during the melatonin treatment period. The individual results of semen analysis were given in our study in Figure 1. In 2 men, we found decreases in sperm concentration and motility that were below the normal range (WHO, 1993). Since the sequence of medications in these subjects was a placebo followed by melatonin, we concluded that the decrease in semen quality was associated with melatonin administration. We also observed an increase in sperm concentration in 3 subjects during melatonin administration. These counts were within the reference range and were not associated with similar changes in sperm motility. We attributed these changes to the well-known variations between samples that exist in the same individual (WHO, 1993). The data presented by Lerchl in the figure describe the average (±SEM) values for sperm concentration for all 8 volunteers examined. It is obvious from our study that, as a group, no trend is seen during melatonin treatment.</p><p>We also determined fasting serum gonadotropins and testosterone and estradiol levels. Although testosterone is secreted in a diurnal fashion (Luboshitzky et al, 2003), a single time point in the morning is sufficient for the assessment of the pituitary-gonadal axis function in men if hormone levels are within the reference range. A recent study has demonstrated that sperm parameters vary with season and advanced age (Chen et al, 2003). These results do not contradict our findings, as we conducted our study between October and May, in a different time zone and in young men.</p><p>We fully agree with the comment that exogenous melatonin influences the diurnal rhythm of the endogenous hormone. In fact, when suitably timed, melatonin administration appears to be beneficial in alleviating symptoms of circadian-based sleep disorders, shift work, jet lag, and delayed sleep phase syndrome as well as a sleep-promoting agent in elderly insomniacs (Zhdanova and Wurtman, 1997; Sack et al, 2000).</p><p>Taken together, the data suggest that exogenous melatonin alters semen quality in some men. Melatonin action at the hypothalamic-pituitary level is less likely in view of unaltered serum gonadotropin levels in our study. A direct inhibitory effect of melatonin on testicular and epididymal aromatase resulting in an altered androgen/estrogen milieu and, consequently, decreased sperm concentration and motility is a more plausible possibility. This is supported by previous observations that low sperm production is associated with low seminal plasma aromatase activity and higher melatonin levels (Yie et al, 1991). Also, in frogs, melatonin has a direct inhibitory effect on the basal- and estradiol-stimulated mitotic activity of primary spermatogonia in the testis (d'Istria et al, 2003).</p><p>In summary, the results of our preliminary study suggest that melatonin decreases sperm counts and motility to subnormal levels in some healthy young men. When considering the long-term use of melatonin, extra precautions should be taken, especially in men with low normal sperm counts.</p>","PeriodicalId":15029,"journal":{"name":"Journal of andrology","volume":"25 2","pages":"185-187"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/j.1939-4640.2004.tb02778.x","citationCount":"15","resultStr":"{\"title\":\"Melatonin Administration Alters Semen Quality in Normal Men\",\"authors\":\"Alexander Lerchl, Rafael Luboshitzky\",\"doi\":\"10.1002/j.1939-4640.2004.tb02778.x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><i>To the Editor</i>:</p><p>The publication by Luboshitzky et al (2002) concerning the effects of melatonin on human sperm quality deserves strong critique for a number of reasons. The authors performed a double-blind crossover study during which healthy volunteers were given either melatonin (3 mg) or a placebo for 3 months each, while between the phases, a washout phase of 2 weeks was included. At the beginning and end of the 2 phases, a total of 11 parameters (sperm and endocrine) were measured and, again, 3 and 6 months after the end of the study. According to the results (!!), volunteers were divided into 2 groups, responders (n = 2) and nonresponders (n = 6). The criterion was that both sperm concentration and sperm motility “dropped during the melatonin treatment period.” Both of these men belonged to the group to which melatonin was given in the second treatment period. The title and the conclusions of this paper are simply not justified by the data for the following reasons:</p><p>In summary, I see no evidence whatsoever for the conclusion that melatonin impairs sperm parameters in healthy men. It rather appears that an expected result influenced the way the data were handled.</p><p><i>To the Editor</i>:</p><p>We appreciate the comments of Lerchl (2004) regarding the effect of exogenous melatonin on sperm quality in normal men (Luboshitzky et al, 2002). In this study, we examined the possible effect of melatonin on semen concentration, motility, and morphology in 8 healthy young men. Since we did not study fertility in the general sense, we performed one semen analysis at baseline. We fully agree that 2 semen samples are indicated for the initial evaluation of fertility. In our study, we defined a subject as a responder if his sperm concentration and motility dropped during the melatonin treatment period. The individual results of semen analysis were given in our study in Figure 1. In 2 men, we found decreases in sperm concentration and motility that were below the normal range (WHO, 1993). Since the sequence of medications in these subjects was a placebo followed by melatonin, we concluded that the decrease in semen quality was associated with melatonin administration. We also observed an increase in sperm concentration in 3 subjects during melatonin administration. These counts were within the reference range and were not associated with similar changes in sperm motility. We attributed these changes to the well-known variations between samples that exist in the same individual (WHO, 1993). The data presented by Lerchl in the figure describe the average (±SEM) values for sperm concentration for all 8 volunteers examined. It is obvious from our study that, as a group, no trend is seen during melatonin treatment.</p><p>We also determined fasting serum gonadotropins and testosterone and estradiol levels. Although testosterone is secreted in a diurnal fashion (Luboshitzky et al, 2003), a single time point in the morning is sufficient for the assessment of the pituitary-gonadal axis function in men if hormone levels are within the reference range. A recent study has demonstrated that sperm parameters vary with season and advanced age (Chen et al, 2003). These results do not contradict our findings, as we conducted our study between October and May, in a different time zone and in young men.</p><p>We fully agree with the comment that exogenous melatonin influences the diurnal rhythm of the endogenous hormone. In fact, when suitably timed, melatonin administration appears to be beneficial in alleviating symptoms of circadian-based sleep disorders, shift work, jet lag, and delayed sleep phase syndrome as well as a sleep-promoting agent in elderly insomniacs (Zhdanova and Wurtman, 1997; Sack et al, 2000).</p><p>Taken together, the data suggest that exogenous melatonin alters semen quality in some men. Melatonin action at the hypothalamic-pituitary level is less likely in view of unaltered serum gonadotropin levels in our study. A direct inhibitory effect of melatonin on testicular and epididymal aromatase resulting in an altered androgen/estrogen milieu and, consequently, decreased sperm concentration and motility is a more plausible possibility. This is supported by previous observations that low sperm production is associated with low seminal plasma aromatase activity and higher melatonin levels (Yie et al, 1991). Also, in frogs, melatonin has a direct inhibitory effect on the basal- and estradiol-stimulated mitotic activity of primary spermatogonia in the testis (d'Istria et al, 2003).</p><p>In summary, the results of our preliminary study suggest that melatonin decreases sperm counts and motility to subnormal levels in some healthy young men. When considering the long-term use of melatonin, extra precautions should be taken, especially in men with low normal sperm counts.</p>\",\"PeriodicalId\":15029,\"journal\":{\"name\":\"Journal of andrology\",\"volume\":\"25 2\",\"pages\":\"185-187\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/j.1939-4640.2004.tb02778.x\",\"citationCount\":\"15\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of andrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/j.1939-4640.2004.tb02778.x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of andrology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/j.1939-4640.2004.tb02778.x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 15
摘要
致编辑:Luboshitzky等人(2002)发表的关于褪黑激素对人类精子质量影响的文章值得强烈批评,原因有很多。作者进行了一项双盲交叉研究,在此期间,健康志愿者分别给予褪黑素(3毫克)或安慰剂3个月,而在两个阶段之间,包括2周的洗脱期。在两个阶段的开始和结束时,共测量了11项参数(精子和内分泌),并在研究结束后的3个月和6个月再次测量。根据结果(!!),志愿者被分为两组,有反应的(n = 2)和无反应的(n = 6)。标准是精子浓度和精子活力“在褪黑激素治疗期间下降”。这两名男性都属于在第二个治疗期给予褪黑素的那一组。这篇论文的标题和结论根本不能被数据所证明,原因如下:总之,我没有看到任何证据表明褪黑激素会损害健康男性的精子参数。更确切地说,似乎预期的结果影响了处理数据的方式。致编辑:我们感谢Lerchl(2004)关于外源褪黑激素对正常男性精子质量影响的评论(Luboshitzky et al, 2002)。在这项研究中,我们研究了褪黑素对8名健康年轻男性精液浓度、活力和形态的可能影响。由于我们没有研究一般意义上的生育能力,我们在基线上进行了一次精液分析。我们完全同意2个精液样本用于生育能力的初步评估。在我们的研究中,如果受试者的精子浓度和活力在褪黑激素治疗期间下降,我们将其定义为应答者。精液分析的个体结果在我们的研究中给出了图1。在2名男性中,我们发现精子浓度和活力低于正常范围(WHO, 1993)。由于这些受试者的用药顺序是安慰剂和褪黑激素,我们得出结论,精液质量的下降与褪黑激素的服用有关。我们还观察到,在服用褪黑激素期间,3名受试者的精子浓度有所增加。这些计数在参考范围内,与精子活力的类似变化无关。我们将这些变化归因于同一个体中存在的样本之间众所周知的差异(世卫组织,1993年)。Lerchl在图中提供的数据描述了所有8名志愿者精子浓度的平均值(±SEM)值。从我们的研究中可以明显看出,作为一个群体,在褪黑激素治疗期间没有看到趋势。我们还测定了空腹血清促性腺激素、睾酮和雌二醇水平。虽然睾酮是按昼夜节律分泌的(Luboshitzky et al, 2003),但如果激素水平在参考范围内,则早晨的单个时间点足以评估男性垂体-性腺轴功能。最近的一项研究表明,精子参数随着季节和年龄的增长而变化(Chen et al, 2003)。这些结果与我们的发现并不矛盾,因为我们的研究是在10月到5月之间进行的,在不同的时区,在年轻男性中进行的。我们完全同意外源性褪黑激素影响内源性激素的昼夜节律的评论。事实上,在适当的时间,褪黑激素的管理似乎有利于缓解昼夜节律睡眠障碍,倒班工作,时差和睡眠阶段延迟综合征的症状,以及老年失眠症的睡眠促进剂(Zhdanova和Wurtman, 1997;Sack et al, 2000)。综上所述,这些数据表明外源性褪黑激素会改变一些男性的精液质量。在我们的研究中,鉴于血清促性腺激素水平不变,褪黑素在下丘脑-垂体水平的作用不太可能。褪黑素对睾丸和附睾芳香酶的直接抑制作用导致雄激素/雌激素环境的改变,从而降低精子浓度和活力是一种更合理的可能性。先前的观察结果支持了这一点,即精子产量低与精浆芳香酶活性低和褪黑素水平高有关(ye et al ., 1991)。此外,在青蛙中,褪黑激素对睾丸中基础和雌二醇刺激的初级精原细胞有丝分裂活性有直接抑制作用(d'Istria等,2003)。总之,我们的初步研究结果表明,褪黑激素会使一些健康年轻男性的精子数量和活力降低到低于正常水平。在考虑长期使用褪黑激素时,应采取额外的预防措施,特别是在正常精子数量较低的男性中。
Melatonin Administration Alters Semen Quality in Normal Men
To the Editor:
The publication by Luboshitzky et al (2002) concerning the effects of melatonin on human sperm quality deserves strong critique for a number of reasons. The authors performed a double-blind crossover study during which healthy volunteers were given either melatonin (3 mg) or a placebo for 3 months each, while between the phases, a washout phase of 2 weeks was included. At the beginning and end of the 2 phases, a total of 11 parameters (sperm and endocrine) were measured and, again, 3 and 6 months after the end of the study. According to the results (!!), volunteers were divided into 2 groups, responders (n = 2) and nonresponders (n = 6). The criterion was that both sperm concentration and sperm motility “dropped during the melatonin treatment period.” Both of these men belonged to the group to which melatonin was given in the second treatment period. The title and the conclusions of this paper are simply not justified by the data for the following reasons:
In summary, I see no evidence whatsoever for the conclusion that melatonin impairs sperm parameters in healthy men. It rather appears that an expected result influenced the way the data were handled.
To the Editor:
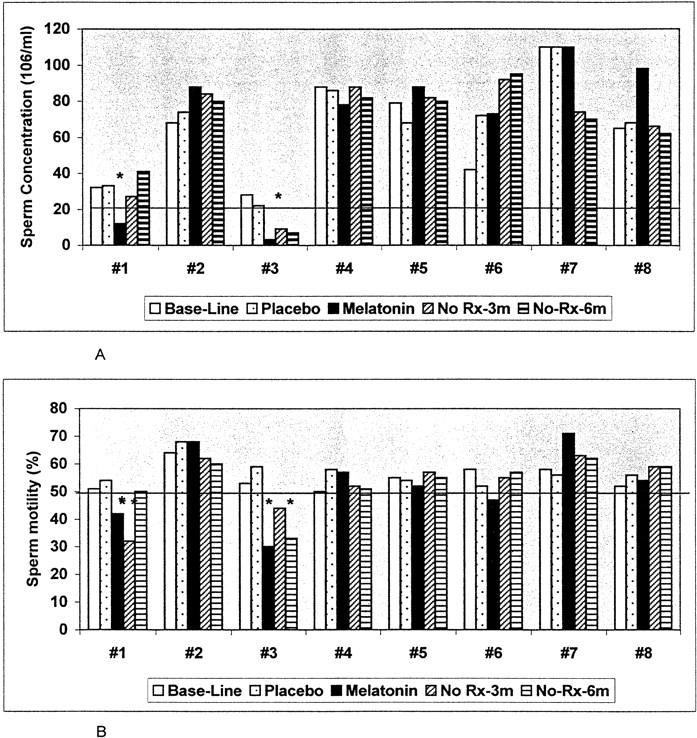
We appreciate the comments of Lerchl (2004) regarding the effect of exogenous melatonin on sperm quality in normal men (Luboshitzky et al, 2002). In this study, we examined the possible effect of melatonin on semen concentration, motility, and morphology in 8 healthy young men. Since we did not study fertility in the general sense, we performed one semen analysis at baseline. We fully agree that 2 semen samples are indicated for the initial evaluation of fertility. In our study, we defined a subject as a responder if his sperm concentration and motility dropped during the melatonin treatment period. The individual results of semen analysis were given in our study in Figure 1. In 2 men, we found decreases in sperm concentration and motility that were below the normal range (WHO, 1993). Since the sequence of medications in these subjects was a placebo followed by melatonin, we concluded that the decrease in semen quality was associated with melatonin administration. We also observed an increase in sperm concentration in 3 subjects during melatonin administration. These counts were within the reference range and were not associated with similar changes in sperm motility. We attributed these changes to the well-known variations between samples that exist in the same individual (WHO, 1993). The data presented by Lerchl in the figure describe the average (±SEM) values for sperm concentration for all 8 volunteers examined. It is obvious from our study that, as a group, no trend is seen during melatonin treatment.
We also determined fasting serum gonadotropins and testosterone and estradiol levels. Although testosterone is secreted in a diurnal fashion (Luboshitzky et al, 2003), a single time point in the morning is sufficient for the assessment of the pituitary-gonadal axis function in men if hormone levels are within the reference range. A recent study has demonstrated that sperm parameters vary with season and advanced age (Chen et al, 2003). These results do not contradict our findings, as we conducted our study between October and May, in a different time zone and in young men.
We fully agree with the comment that exogenous melatonin influences the diurnal rhythm of the endogenous hormone. In fact, when suitably timed, melatonin administration appears to be beneficial in alleviating symptoms of circadian-based sleep disorders, shift work, jet lag, and delayed sleep phase syndrome as well as a sleep-promoting agent in elderly insomniacs (Zhdanova and Wurtman, 1997; Sack et al, 2000).
Taken together, the data suggest that exogenous melatonin alters semen quality in some men. Melatonin action at the hypothalamic-pituitary level is less likely in view of unaltered serum gonadotropin levels in our study. A direct inhibitory effect of melatonin on testicular and epididymal aromatase resulting in an altered androgen/estrogen milieu and, consequently, decreased sperm concentration and motility is a more plausible possibility. This is supported by previous observations that low sperm production is associated with low seminal plasma aromatase activity and higher melatonin levels (Yie et al, 1991). Also, in frogs, melatonin has a direct inhibitory effect on the basal- and estradiol-stimulated mitotic activity of primary spermatogonia in the testis (d'Istria et al, 2003).
In summary, the results of our preliminary study suggest that melatonin decreases sperm counts and motility to subnormal levels in some healthy young men. When considering the long-term use of melatonin, extra precautions should be taken, especially in men with low normal sperm counts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


