Martin Christa, Brendan Smyth, Kaitlin J Mayne, Stefano Stuard, Bernard Canaud, Bernd Genser, Jule Pinter
{"title":"血液透析患者累积暴露于液体过载和透析液钠≤138 mmol/l时心脏死亡风险增加","authors":"Martin Christa, Brendan Smyth, Kaitlin J Mayne, Stefano Stuard, Bernard Canaud, Bernd Genser, Jule Pinter","doi":"10.1093/ckj/sfaf259","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fluid overload (FO) is an established risk factor for mortality in hemodialysis patients, who face higher cardiovascular mortality risk than the general population. Despite the known impact of FO on cardiovascular outcomes, the effects of cumulative FO exposure, dialysate sodium ≤138 mmol/l, and specific cardiac deaths remain unclear. This study aimed to assess these relationships in a large cohort of hemodialysis patients.</p><p><strong>Methods: </strong>This historical cohort study included 68 196 hemodialysis patients from the NephroCare network with data from 2010 to 2019. Eligible patients had valid bioimpedance, plasma, and dialysate sodium measurements within 90 days of starting hemodialysis. FO was defined as >7% relative FO, as assessed by bioimpedance spectroscopy. Cause-specific Cox proportional hazards models were used to evaluate the impact of these exposures on different cardiac endpoints, including death from heart failure, sudden cardiac death, and fatal myocardial infarction.</p><p><strong>Results: </strong>In 68 196 patients, a total of 2 123 957 patient-months were analyzed. Compared to patients with no prior exposure (0 month cumulative past exposure time), increasing cumulative exposure to FO (measured in months) significantly increased the risk of death from heart failure [hazard ratio (HR) peaking at 4.4, 95%CI: 3.4-5.6], sudden cardiac death (HR peaking at 4.0, 95%CI: 3.1-5.2), and fatal myocardial infarction (HR peaking at 3.3, 95%CI: 2.5-4.4). Cumulative exposure (in month) to dialysate sodium ≤138 mmol/l was associated with an elevated risk of death from heart failure (HR peaking at 6.0, 95%CI: 1.9-18.3) and a moderate increase in sudden cardiac death (HR peaking at 2.7, 95%CI: 1.3-5.6). The risk of all-cause mortality was consistently higher in patients exposed to FO (HR peaking at 3.4, 95%CI: 3.1-3.8) and those exposed to dialysate sodium ≤138 mmol/l (HR peaking at 2.0, 95%CI: 1.3-3.1).</p><p><strong>Conclusion: </strong>Cumulative FO and dialysate sodium ≤138 mmol/l significantly increase cardiac death risk in hemodialysis patients, particularly from heart failure. Stringent fluid management and careful consideration of dialysate sodium prescription is crucial to reduce cardiovascular mortality.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 10","pages":"sfaf259"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12541371/pdf/","citationCount":"0","resultStr":"{\"title\":\"Increased risk of cardiac death with cumulative exposure to fluid overload and dialysate sodium ≤138 mmol/l in hemodialysis patients.\",\"authors\":\"Martin Christa, Brendan Smyth, Kaitlin J Mayne, Stefano Stuard, Bernard Canaud, Bernd Genser, Jule Pinter\",\"doi\":\"10.1093/ckj/sfaf259\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fluid overload (FO) is an established risk factor for mortality in hemodialysis patients, who face higher cardiovascular mortality risk than the general population. Despite the known impact of FO on cardiovascular outcomes, the effects of cumulative FO exposure, dialysate sodium ≤138 mmol/l, and specific cardiac deaths remain unclear. This study aimed to assess these relationships in a large cohort of hemodialysis patients.</p><p><strong>Methods: </strong>This historical cohort study included 68 196 hemodialysis patients from the NephroCare network with data from 2010 to 2019. Eligible patients had valid bioimpedance, plasma, and dialysate sodium measurements within 90 days of starting hemodialysis. FO was defined as >7% relative FO, as assessed by bioimpedance spectroscopy. Cause-specific Cox proportional hazards models were used to evaluate the impact of these exposures on different cardiac endpoints, including death from heart failure, sudden cardiac death, and fatal myocardial infarction.</p><p><strong>Results: </strong>In 68 196 patients, a total of 2 123 957 patient-months were analyzed. Compared to patients with no prior exposure (0 month cumulative past exposure time), increasing cumulative exposure to FO (measured in months) significantly increased the risk of death from heart failure [hazard ratio (HR) peaking at 4.4, 95%CI: 3.4-5.6], sudden cardiac death (HR peaking at 4.0, 95%CI: 3.1-5.2), and fatal myocardial infarction (HR peaking at 3.3, 95%CI: 2.5-4.4). Cumulative exposure (in month) to dialysate sodium ≤138 mmol/l was associated with an elevated risk of death from heart failure (HR peaking at 6.0, 95%CI: 1.9-18.3) and a moderate increase in sudden cardiac death (HR peaking at 2.7, 95%CI: 1.3-5.6). The risk of all-cause mortality was consistently higher in patients exposed to FO (HR peaking at 3.4, 95%CI: 3.1-3.8) and those exposed to dialysate sodium ≤138 mmol/l (HR peaking at 2.0, 95%CI: 1.3-3.1).</p><p><strong>Conclusion: </strong>Cumulative FO and dialysate sodium ≤138 mmol/l significantly increase cardiac death risk in hemodialysis patients, particularly from heart failure. Stringent fluid management and careful consideration of dialysate sodium prescription is crucial to reduce cardiovascular mortality.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 10\",\"pages\":\"sfaf259\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12541371/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf259\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf259","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Increased risk of cardiac death with cumulative exposure to fluid overload and dialysate sodium ≤138 mmol/l in hemodialysis patients.
Background: Fluid overload (FO) is an established risk factor for mortality in hemodialysis patients, who face higher cardiovascular mortality risk than the general population. Despite the known impact of FO on cardiovascular outcomes, the effects of cumulative FO exposure, dialysate sodium ≤138 mmol/l, and specific cardiac deaths remain unclear. This study aimed to assess these relationships in a large cohort of hemodialysis patients.
Methods: This historical cohort study included 68 196 hemodialysis patients from the NephroCare network with data from 2010 to 2019. Eligible patients had valid bioimpedance, plasma, and dialysate sodium measurements within 90 days of starting hemodialysis. FO was defined as >7% relative FO, as assessed by bioimpedance spectroscopy. Cause-specific Cox proportional hazards models were used to evaluate the impact of these exposures on different cardiac endpoints, including death from heart failure, sudden cardiac death, and fatal myocardial infarction.
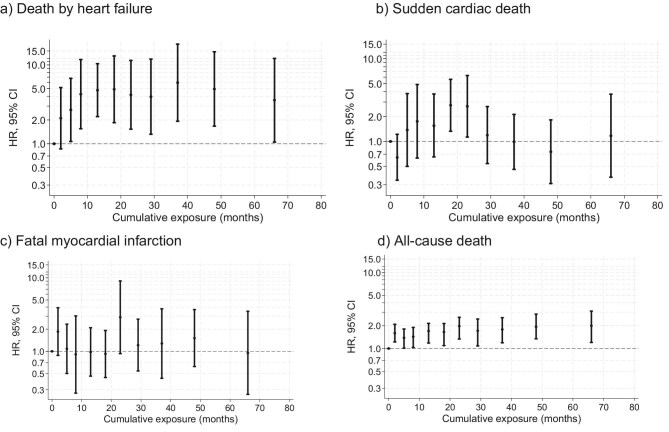
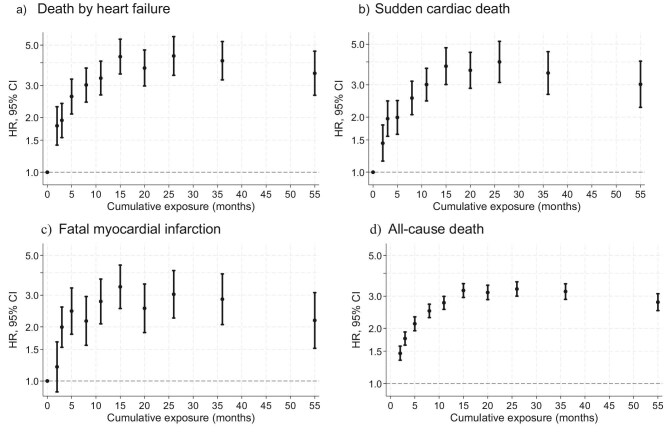
Results: In 68 196 patients, a total of 2 123 957 patient-months were analyzed. Compared to patients with no prior exposure (0 month cumulative past exposure time), increasing cumulative exposure to FO (measured in months) significantly increased the risk of death from heart failure [hazard ratio (HR) peaking at 4.4, 95%CI: 3.4-5.6], sudden cardiac death (HR peaking at 4.0, 95%CI: 3.1-5.2), and fatal myocardial infarction (HR peaking at 3.3, 95%CI: 2.5-4.4). Cumulative exposure (in month) to dialysate sodium ≤138 mmol/l was associated with an elevated risk of death from heart failure (HR peaking at 6.0, 95%CI: 1.9-18.3) and a moderate increase in sudden cardiac death (HR peaking at 2.7, 95%CI: 1.3-5.6). The risk of all-cause mortality was consistently higher in patients exposed to FO (HR peaking at 3.4, 95%CI: 3.1-3.8) and those exposed to dialysate sodium ≤138 mmol/l (HR peaking at 2.0, 95%CI: 1.3-3.1).
Conclusion: Cumulative FO and dialysate sodium ≤138 mmol/l significantly increase cardiac death risk in hemodialysis patients, particularly from heart failure. Stringent fluid management and careful consideration of dialysate sodium prescription is crucial to reduce cardiovascular mortality.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


