Katarzyna Gąsowska, Katarzyna Zachwieja, Monika Miklaszewska, Aleksandra Krasowska-Kwiecień, Jolanta Goździk, Dorota Drożdż
{"title":"儿童造血干细胞移植受者慢性肾脏疾病的5年观察-单中心经验","authors":"Katarzyna Gąsowska, Katarzyna Zachwieja, Monika Miklaszewska, Aleksandra Krasowska-Kwiecień, Jolanta Goździk, Dorota Drożdż","doi":"10.1155/ijpe/5335429","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic kidney disease (CKD) is a common complication of hematopoietic stem cell transplantation (HSCT). However, the data on its risk factors in the pediatric population is conflicting.</p><p><strong>Methods: </strong>We retrospectively analyzed data from HSCT patients treated between 2005 and 2019, including indications for HSCT, conditioning regimens, and complications observed during a 5-year follow-up period, and calculated estimated glomerular filtration rate (eGFR) values. We used repeated measures ANOVA to model the time course of eGFR as a function of CKD. We built unadjusted and multiple adjusted logistic regression models. We did Kaplan-Meier plots and Cox regression with CKD as a potential risk factor for mortality.</p><p><strong>Results: </strong>At HSCT, the median age (q5-q95) of the 200 (33.5% female) patients was 8.3 (0.64-17.4) years, median creatinine was 33.8 (17.0-65.5) <i>μ</i>mol/L, 49 (24.5%) developed CKD, and 42 (21.0%) died during follow-up. In the unadjusted logistic regression model, CKD was negatively related to baseline eGFR (unadjusted OR per 10 mL/min/1.73 m<sup>2</sup> greater eGFR: 0.87, 95% CI 0.78-0.95; <i>p</i> = 0.004). In the stepwise selection model, greater AKI severity (OR 2.92, 95% CI 1.89-4.15; <i>p</i> < 0.0001), presence of hypertension (OR 2.68, 95% CI 1.02-7.05; <i>p</i> = 0.05), malnutrition (OR 5.42, 95% CI 1.98-14.82; <i>p</i> = 0.001), and iron overload (OR 3.88, 95% CI 1.31-11.51; <i>p</i> = 0.01) were related to CKD during follow-up. Female sex was protective (OR 0.19, 95% CI 0.06-0.61; <i>p</i> = 0.005). CKD status during follow-up was not related to the risk of mortality.</p><p><strong>Conclusion: </strong>Our results underline the need for better nutrition, prevention of iron overload, and adequate blood pressure control to prevent CKD in pediatric patients after HSCT.</p>","PeriodicalId":51591,"journal":{"name":"International Journal of Pediatrics","volume":"2025 ","pages":"5335429"},"PeriodicalIF":1.3000,"publicationDate":"2025-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12540005/pdf/","citationCount":"0","resultStr":"{\"title\":\"Chronic Kidney Disease in Pediatric Recipients of Hematopoietic Stem Cell Transplantation in a 5-Year Observation-A Single Center Experience.\",\"authors\":\"Katarzyna Gąsowska, Katarzyna Zachwieja, Monika Miklaszewska, Aleksandra Krasowska-Kwiecień, Jolanta Goździk, Dorota Drożdż\",\"doi\":\"10.1155/ijpe/5335429\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronic kidney disease (CKD) is a common complication of hematopoietic stem cell transplantation (HSCT). However, the data on its risk factors in the pediatric population is conflicting.</p><p><strong>Methods: </strong>We retrospectively analyzed data from HSCT patients treated between 2005 and 2019, including indications for HSCT, conditioning regimens, and complications observed during a 5-year follow-up period, and calculated estimated glomerular filtration rate (eGFR) values. We used repeated measures ANOVA to model the time course of eGFR as a function of CKD. We built unadjusted and multiple adjusted logistic regression models. We did Kaplan-Meier plots and Cox regression with CKD as a potential risk factor for mortality.</p><p><strong>Results: </strong>At HSCT, the median age (q5-q95) of the 200 (33.5% female) patients was 8.3 (0.64-17.4) years, median creatinine was 33.8 (17.0-65.5) <i>μ</i>mol/L, 49 (24.5%) developed CKD, and 42 (21.0%) died during follow-up. In the unadjusted logistic regression model, CKD was negatively related to baseline eGFR (unadjusted OR per 10 mL/min/1.73 m<sup>2</sup> greater eGFR: 0.87, 95% CI 0.78-0.95; <i>p</i> = 0.004). In the stepwise selection model, greater AKI severity (OR 2.92, 95% CI 1.89-4.15; <i>p</i> < 0.0001), presence of hypertension (OR 2.68, 95% CI 1.02-7.05; <i>p</i> = 0.05), malnutrition (OR 5.42, 95% CI 1.98-14.82; <i>p</i> = 0.001), and iron overload (OR 3.88, 95% CI 1.31-11.51; <i>p</i> = 0.01) were related to CKD during follow-up. Female sex was protective (OR 0.19, 95% CI 0.06-0.61; <i>p</i> = 0.005). CKD status during follow-up was not related to the risk of mortality.</p><p><strong>Conclusion: </strong>Our results underline the need for better nutrition, prevention of iron overload, and adequate blood pressure control to prevent CKD in pediatric patients after HSCT.</p>\",\"PeriodicalId\":51591,\"journal\":{\"name\":\"International Journal of Pediatrics\",\"volume\":\"2025 \",\"pages\":\"5335429\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-10-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12540005/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/ijpe/5335429\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/ijpe/5335429","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:慢性肾脏疾病(CKD)是造血干细胞移植(HSCT)的常见并发症。然而,关于儿童人群的风险因素的数据是相互矛盾的。方法:回顾性分析2005年至2019年接受HSCT治疗的患者数据,包括5年随访期间观察到的HSCT适应症、调理方案和并发症,并计算肾小球滤过率(eGFR)估计值。我们使用重复测量方差分析来模拟eGFR的时间过程作为CKD的函数。我们建立了未调整和多调整的逻辑回归模型。我们将CKD作为死亡率的潜在危险因素进行了Kaplan-Meier图和Cox回归分析。结果:在HSCT中,200例患者(33.5%为女性)的中位年龄(q5-q95)为8.3(0.64-17.4)岁,中位肌酐为33.8 (17.0-65.5)μmol/L, 49例(24.5%)发生CKD, 42例(21.0%)在随访中死亡。在未经调整的logistic回归模型中,CKD与基线eGFR呈负相关(未经调整的OR每10 mL/min/1.73 m2 eGFR增加:0.87,95% CI 0.78-0.95; p = 0.004)。在逐步选择模型中,随访期间,较高的AKI严重程度(OR 2.92, 95% CI 1.89-4.15, p < 0.0001)、高血压(OR 2.68, 95% CI 1.02-7.05, p = 0.05)、营养不良(OR 5.42, 95% CI 1.98-14.82, p = 0.001)和铁超载(OR 3.88, 95% CI 1.31-11.51, p = 0.01)与CKD相关。女性具有保护作用(OR 0.19, 95% CI 0.06-0.61; p = 0.005)。随访期间CKD状态与死亡风险无关。结论:我们的研究结果强调,需要更好的营养,预防铁超载,适当的血压控制,以防止儿童肾移植后CKD的发生。
Chronic Kidney Disease in Pediatric Recipients of Hematopoietic Stem Cell Transplantation in a 5-Year Observation-A Single Center Experience.
Background: Chronic kidney disease (CKD) is a common complication of hematopoietic stem cell transplantation (HSCT). However, the data on its risk factors in the pediatric population is conflicting.
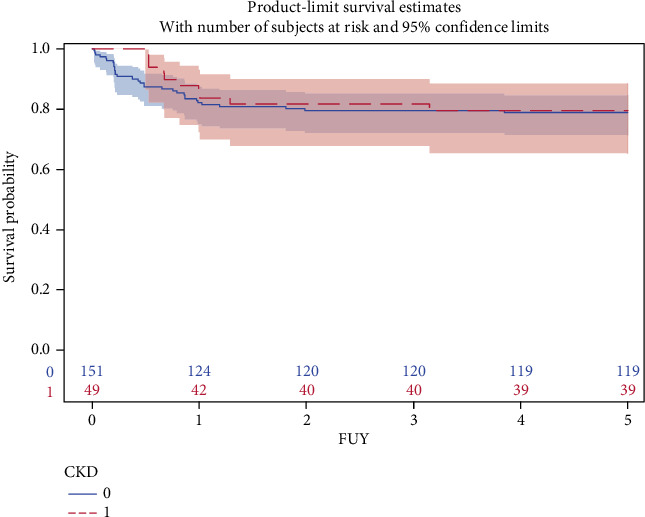
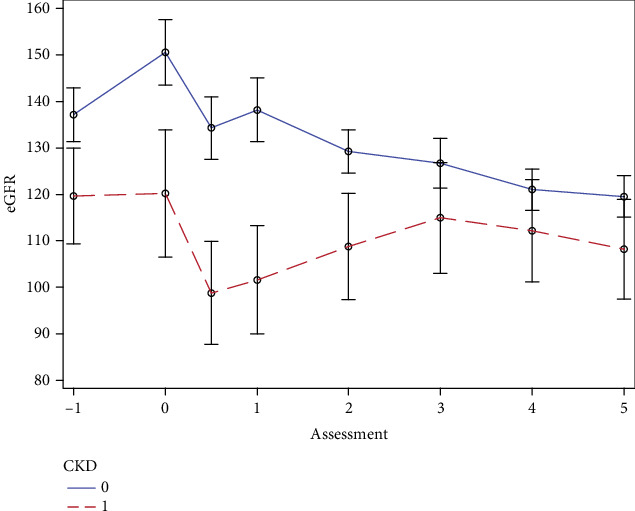
Methods: We retrospectively analyzed data from HSCT patients treated between 2005 and 2019, including indications for HSCT, conditioning regimens, and complications observed during a 5-year follow-up period, and calculated estimated glomerular filtration rate (eGFR) values. We used repeated measures ANOVA to model the time course of eGFR as a function of CKD. We built unadjusted and multiple adjusted logistic regression models. We did Kaplan-Meier plots and Cox regression with CKD as a potential risk factor for mortality.
Results: At HSCT, the median age (q5-q95) of the 200 (33.5% female) patients was 8.3 (0.64-17.4) years, median creatinine was 33.8 (17.0-65.5) μmol/L, 49 (24.5%) developed CKD, and 42 (21.0%) died during follow-up. In the unadjusted logistic regression model, CKD was negatively related to baseline eGFR (unadjusted OR per 10 mL/min/1.73 m2 greater eGFR: 0.87, 95% CI 0.78-0.95; p = 0.004). In the stepwise selection model, greater AKI severity (OR 2.92, 95% CI 1.89-4.15; p < 0.0001), presence of hypertension (OR 2.68, 95% CI 1.02-7.05; p = 0.05), malnutrition (OR 5.42, 95% CI 1.98-14.82; p = 0.001), and iron overload (OR 3.88, 95% CI 1.31-11.51; p = 0.01) were related to CKD during follow-up. Female sex was protective (OR 0.19, 95% CI 0.06-0.61; p = 0.005). CKD status during follow-up was not related to the risk of mortality.
Conclusion: Our results underline the need for better nutrition, prevention of iron overload, and adequate blood pressure control to prevent CKD in pediatric patients after HSCT.
期刊介绍:
International Journal of Pediatrics is a peer-reviewed, open access journal that publishes original researcharticles, review articles, and clinical studies in all areas of pediatric research. The journal accepts submissions presented as an original article, short communication, case report, review article, systematic review, or letter to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


