{"title":"多模式脑监测引导麻醉管理改善功能连通性,促进恢复和减轻老年外科患者术后疼痛。","authors":"Shuyi Yang, Shuai Feng, Hao Wu, Chonglin Zhong, Shubin Zhan, Chunxiu Wang, Zan Chen, Yaxian Huang, Guanxu Zhao, Yue Zhang, Tianlong Wang, Wei Xiao","doi":"10.2147/CIA.S551727","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.</p><p><strong>Patients and methods: </strong>Patients (aged ≥65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).</p><p><strong>Results: </strong>Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (<i>P</i> < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: <i>P</i>=0.04; 24h: <i>P</i>=0.04) and during movement (1h: <i>P</i>=0.03).</p><p><strong>Conclusion: </strong>These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.</p>","PeriodicalId":48841,"journal":{"name":"Clinical Interventions in Aging","volume":"20 ","pages":"1757-1771"},"PeriodicalIF":3.7000,"publicationDate":"2025-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12535745/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multimodal Brain Monitoring-Guided Anesthesia Management Improves Functional Connectivity, Enhances Recovery and Attenuates Postoperative Pain in Elderly Surgical Patients.\",\"authors\":\"Shuyi Yang, Shuai Feng, Hao Wu, Chonglin Zhong, Shubin Zhan, Chunxiu Wang, Zan Chen, Yaxian Huang, Guanxu Zhao, Yue Zhang, Tianlong Wang, Wei Xiao\",\"doi\":\"10.2147/CIA.S551727\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.</p><p><strong>Patients and methods: </strong>Patients (aged ≥65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).</p><p><strong>Results: </strong>Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (<i>P</i> < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: <i>P</i>=0.04; 24h: <i>P</i>=0.04) and during movement (1h: <i>P</i>=0.03).</p><p><strong>Conclusion: </strong>These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.</p>\",\"PeriodicalId\":48841,\"journal\":{\"name\":\"Clinical Interventions in Aging\",\"volume\":\"20 \",\"pages\":\"1757-1771\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2025-10-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12535745/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Interventions in Aging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CIA.S551727\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Interventions in Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CIA.S551727","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:围手术期神经认知障碍(PND)在老年外科患者中较为常见,严重影响术后恢复。然而,仍然缺乏有效的预防措施。围手术期潜在的脑应激源(包括不适当的镇静/镇痛深度和不平衡的脑氧供需)可能是重要的影响因素。我们制定了一种基于多模式脑监测的麻醉管理方案,以实现镇静/镇痛深度和脑氧饱和度的标准化、个体化和实时调节,并研究它是否可以降低PND的发生率及其潜在机制。患者和方法:年龄≥65岁的患者随机分为C组(n=88)和E组(n=93)。E组采用多模式脑监测引导麻醉管理,C组采用bis引导麻醉管理。术前和术后7天分别进行蒙特利尔认知评估(MoCA)。记录术后疼痛评分。分析静息状态功能MRI数据以检查功能连接(FC)。结果:E组PND的发生率较低(15.50% vs 21.59%),但差异无统计学意义。E组患者右侧枕后区、右侧回下区、右侧顶叶下小叶FC增高(P < 0.05)。E组静息时(1h: P=0.04; 24h: P=0.04)和运动时(1h: P=0.03)疼痛评分明显低于对照组。结论:这些结果表明,多模式脑监测引导麻醉管理可能通过增强认知相关脑区的FC和减轻术后急性疼痛来保护神经认知。在老年外科患者中,与bis引导的麻醉管理相比,多模式脑监测引导的麻醉管理可能会降低PND的发生率。
Multimodal Brain Monitoring-Guided Anesthesia Management Improves Functional Connectivity, Enhances Recovery and Attenuates Postoperative Pain in Elderly Surgical Patients.
Purpose: Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.
Patients and methods: Patients (aged ≥65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).
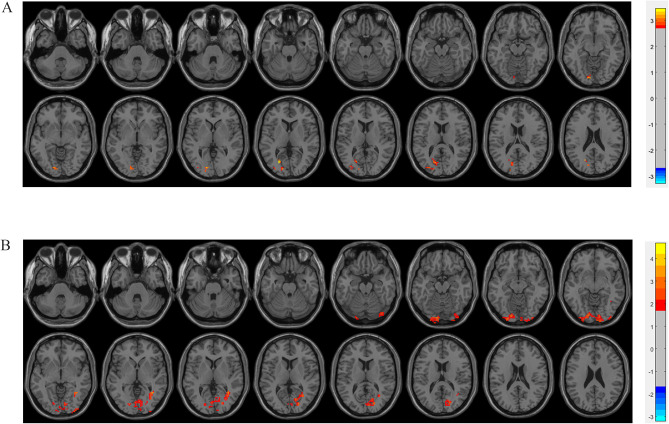
Results: Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (P < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: P=0.04; 24h: P=0.04) and during movement (1h: P=0.03).
Conclusion: These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.
期刊介绍:
Clinical Interventions in Aging, is an online, peer reviewed, open access journal focusing on concise rapid reporting of original research and reviews in aging. Special attention will be given to papers reporting on actual or potential clinical applications leading to improved prevention or treatment of disease or a greater understanding of pathological processes that result from maladaptive changes in the body associated with aging. This journal is directed at a wide array of scientists, engineers, pharmacists, pharmacologists and clinical specialists wishing to maintain an up to date knowledge of this exciting and emerging field.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


