Vaishnavi Thevrekandy, Aravind Sreekumar, Praveen Aggarwal, Jamshed Nayer, K R Sanith
{"title":"急诊住院时间与住院死亡率:一项前瞻性观察研究。","authors":"Vaishnavi Thevrekandy, Aravind Sreekumar, Praveen Aggarwal, Jamshed Nayer, K R Sanith","doi":"10.4103/tjem.tjem_97_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We aimed to study the association between prolonged boarding time in the emergency department (ED) and in-hospital mortality among patients triaged red at presentation.</p><p><strong>Methods: </strong>It was a single-center prospective observational study conducted among 300 patients who presented to the ED of a tertiary care teaching institute in North India. The boarding time was calculated as the time interval between the time at which the patient was advised admission and the time at which the patient was admitted to the indoor bed. Risk stratification of patients was done based on National Early Warning Score 2 (NEWS2) at presentation. The patient was then followed up for the duration of their in-hospital course, till discharge or death.</p><p><strong>Results: </strong>The mean boarding time was higher in patients who died, as compared to those who were alive, but the difference was not found to be statistically significant (14.13 h vs. 11.89 h, <i>P</i> = 0.053). Boarding time had a weak discriminatory power on receiver operating characteristic (ROC) analysis (area under the ROC: 0.59: 95% confidence interval [CI]: 0.51-0.67, <i>P</i> = 0.046). A boarding time of more than 9.98 h was found to be 70.8% specific and 43.6% sensitive for predicting in-hospital mortality. On logistic regression, an increase in boarding time was found to independently increase the odds of mortality, albeit weakly (adjusted odds ratio: 1.06; 95% CI: 1.00-1.12, <i>P</i> = 0.03). A NEWS2 score > 4 at presentation and a requirement of high-dependency unit (HDU)/ıntensive care unit (ICU) admission were found to be significant predictors of in-hospital mortality.</p><p><strong>Conclusion: </strong>Prolonged ED boarding times may be weakly associated with in-hospital mortality. Patients with an increased NEWS2 score at presentation and those requiring HDU/ICU admissions were at higher risk of in-hospital mortality.</p>","PeriodicalId":46536,"journal":{"name":"Turkish Journal of Emergency Medicine","volume":"25 4","pages":"297-304"},"PeriodicalIF":2.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527061/pdf/","citationCount":"0","resultStr":"{\"title\":\"Emergency department boarding time and in-hospital mortality: A prospective observational study.\",\"authors\":\"Vaishnavi Thevrekandy, Aravind Sreekumar, Praveen Aggarwal, Jamshed Nayer, K R Sanith\",\"doi\":\"10.4103/tjem.tjem_97_25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>We aimed to study the association between prolonged boarding time in the emergency department (ED) and in-hospital mortality among patients triaged red at presentation.</p><p><strong>Methods: </strong>It was a single-center prospective observational study conducted among 300 patients who presented to the ED of a tertiary care teaching institute in North India. The boarding time was calculated as the time interval between the time at which the patient was advised admission and the time at which the patient was admitted to the indoor bed. Risk stratification of patients was done based on National Early Warning Score 2 (NEWS2) at presentation. The patient was then followed up for the duration of their in-hospital course, till discharge or death.</p><p><strong>Results: </strong>The mean boarding time was higher in patients who died, as compared to those who were alive, but the difference was not found to be statistically significant (14.13 h vs. 11.89 h, <i>P</i> = 0.053). Boarding time had a weak discriminatory power on receiver operating characteristic (ROC) analysis (area under the ROC: 0.59: 95% confidence interval [CI]: 0.51-0.67, <i>P</i> = 0.046). A boarding time of more than 9.98 h was found to be 70.8% specific and 43.6% sensitive for predicting in-hospital mortality. On logistic regression, an increase in boarding time was found to independently increase the odds of mortality, albeit weakly (adjusted odds ratio: 1.06; 95% CI: 1.00-1.12, <i>P</i> = 0.03). A NEWS2 score > 4 at presentation and a requirement of high-dependency unit (HDU)/ıntensive care unit (ICU) admission were found to be significant predictors of in-hospital mortality.</p><p><strong>Conclusion: </strong>Prolonged ED boarding times may be weakly associated with in-hospital mortality. Patients with an increased NEWS2 score at presentation and those requiring HDU/ICU admissions were at higher risk of in-hospital mortality.</p>\",\"PeriodicalId\":46536,\"journal\":{\"name\":\"Turkish Journal of Emergency Medicine\",\"volume\":\"25 4\",\"pages\":\"297-304\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527061/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Turkish Journal of Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/tjem.tjem_97_25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/tjem.tjem_97_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:我们旨在研究急诊(ED)住院时间延长与就诊时被分类为红色的患者住院死亡率之间的关系。方法:这是一项单中心前瞻性观察研究,在印度北部一家三级护理教学机构的急诊科进行了300例患者的研究。登机时间计算为患者被告知入院时间与患者入住室内床时间之间的时间间隔。患者的风险分层是基于国家早期预警评分2 (NEWS2)。然后对患者进行住院期间的随访,直到出院或死亡。结果:死亡患者的平均登机时间高于存活患者,但差异无统计学意义(14.13 h比11.89 h, P = 0.053)。登机时间对受试者工作特征(ROC)分析有微弱的区别作用(ROC下面积:0.59:95%置信区间[CI]: 0.51-0.67, P = 0.046)。登机时间大于9.98 h对预测住院死亡率的特异性为70.8%,敏感性为43.6%。在逻辑回归中,登机时间的增加独立地增加了死亡率的几率,尽管微弱(调整后的优势比:1.06;95% CI: 1.00-1.12, P = 0.03)。入院时NEWS2评分bbbb4和入住高依赖病房(HDU)/ıntensive护理病房(ICU)的要求被发现是住院死亡率的重要预测因子。结论:延长急诊科登机时间可能与住院死亡率呈弱相关。就诊时NEWS2评分升高的患者和需要HDU/ICU入院的患者在院内死亡的风险更高。
Emergency department boarding time and in-hospital mortality: A prospective observational study.
Objectives: We aimed to study the association between prolonged boarding time in the emergency department (ED) and in-hospital mortality among patients triaged red at presentation.
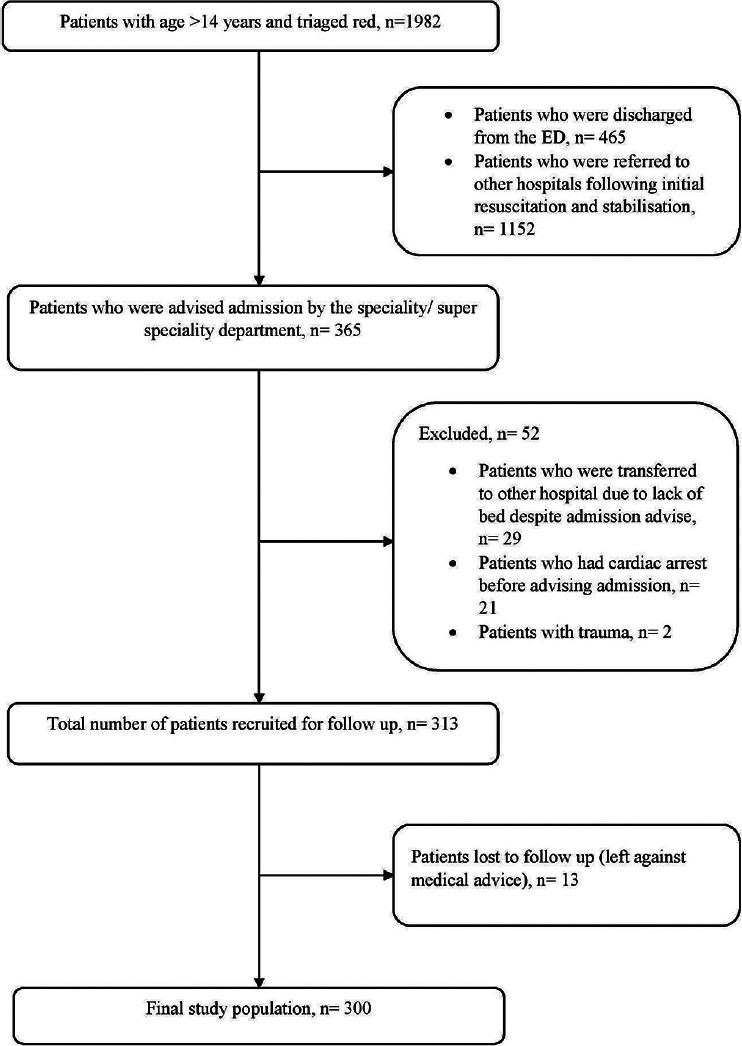
Methods: It was a single-center prospective observational study conducted among 300 patients who presented to the ED of a tertiary care teaching institute in North India. The boarding time was calculated as the time interval between the time at which the patient was advised admission and the time at which the patient was admitted to the indoor bed. Risk stratification of patients was done based on National Early Warning Score 2 (NEWS2) at presentation. The patient was then followed up for the duration of their in-hospital course, till discharge or death.
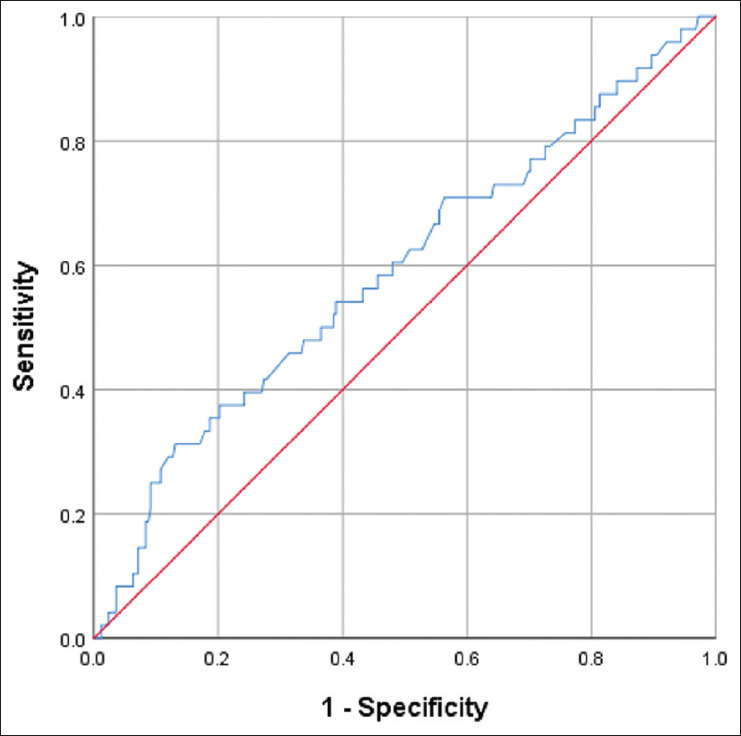
Results: The mean boarding time was higher in patients who died, as compared to those who were alive, but the difference was not found to be statistically significant (14.13 h vs. 11.89 h, P = 0.053). Boarding time had a weak discriminatory power on receiver operating characteristic (ROC) analysis (area under the ROC: 0.59: 95% confidence interval [CI]: 0.51-0.67, P = 0.046). A boarding time of more than 9.98 h was found to be 70.8% specific and 43.6% sensitive for predicting in-hospital mortality. On logistic regression, an increase in boarding time was found to independently increase the odds of mortality, albeit weakly (adjusted odds ratio: 1.06; 95% CI: 1.00-1.12, P = 0.03). A NEWS2 score > 4 at presentation and a requirement of high-dependency unit (HDU)/ıntensive care unit (ICU) admission were found to be significant predictors of in-hospital mortality.
Conclusion: Prolonged ED boarding times may be weakly associated with in-hospital mortality. Patients with an increased NEWS2 score at presentation and those requiring HDU/ICU admissions were at higher risk of in-hospital mortality.
期刊介绍:
The Turkish Journal of Emergency Medicine (Turk J Emerg Med) is an International, peer-reviewed, open-access journal that publishes clinical and experimental trials, case reports, invited reviews, case images, letters to the Editor, and interesting research conducted in all fields of Emergency Medicine. The Journal is the official scientific publication of the Emergency Medicine Association of Turkey (EMAT) and is printed four times a year, in January, April, July and October. The language of the journal is English. The Journal is based on independent and unbiased double-blinded peer-reviewed principles. Only unpublished papers that are not under review for publication elsewhere can be submitted. The authors are responsible for the scientific content of the material to be published. The Turkish Journal of Emergency Medicine reserves the right to request any research materials on which the paper is based. The Editorial Board of the Turkish Journal of Emergency Medicine and the Publisher adheres to the principles of the International Council of Medical Journal Editors, the World Association of Medical Editors, the Council of Science Editors, the Committee on Publication Ethics, the US National Library of Medicine, the US Office of Research Integrity, the European Association of Science Editors, and the International Society of Managing and Technical Editors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


