{"title":"床边肺超声、定量胸部CT和衰弱评估对老年重症肺炎患者短期预后的预测价值:一项初步研究","authors":"Longjiang Shao, Yongyong Liang","doi":"10.1186/s12890-025-03950-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Elderly patients with severe community-acquired pneumonia (CAP) have high short-term mortality, yet conventional severity scores do not incorporate bedside imaging or physiological frailty. In this study we aim to (1) evaluate the feasibility of obtaining lung ultrasound (LUS), quantitative chest computed tomography (CT), and Clinical Frailty Scale (CFS) assessments during the same admission and (2) explore the predictive potential for 28-day mortality by integrating imaging severity with physiological frailty.</p><p><strong>Methods: </strong>In this prospective, single-center pilot study (February 2022 - February 2025), we consecutively enrolled 60 hospitalized adults ≥ 65 years who met guideline criteria for severe CAP and completed 28-day follow-up. Twelve-zone LUS and CFS assessments were performed ≤ 24 h after admission; chest CT was acquired within 48 h when clinically permissible. Feasibility outcomes were recruitment rate, data completeness, and study-related adverse events. Associations with 28-day mortality were analyzed descriptively and with exploratory multivariable logistic regression.</p><p><strong>Results: </strong>LUS and CFS were completed in 100% and 93.3% of participants, respectively; CT was obtained in 83.3%. No study-related adverse events occurred. Twelve patients (20%) died within 28 days. Compared with survivors, non-survivors had higher median LUS scores (14.1 vs. 12.1), greater CT-defined consolidation (30% vs. 22% of lung volume), and a higher prevalence of severe frailty (58% vs. 25%). In the 50 participants with complete data, both LUS score (odds ratio [OR] 1.09 per point) and severe frailty (OR 3.85) independently predicted mortality. A model combining LUS and frailty improved discrimination relative to CURB-65 alone (area under the receiver-operating characteristic curve 0.75 vs. 0.68).</p><p><strong>Conclusions: </strong>Simultaneous acquisition of LUS, quantitative CT, and frailty metrics is feasible, safe, and well tolerated in elderly patients with severe CAP. Preliminary evidence suggests that integrating imaging severity with physiological frailty enhances short-term risk stratification beyond established clinical scores. These findings merit confirmation in larger, multicenter cohorts.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"474"},"PeriodicalIF":2.8000,"publicationDate":"2025-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12522310/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictive value of bedside lung ultrasound, quantitative chest CT, and frailty assessment for short-term outcomes in elderly patients with severe pneumonia: a pilot study.\",\"authors\":\"Longjiang Shao, Yongyong Liang\",\"doi\":\"10.1186/s12890-025-03950-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Elderly patients with severe community-acquired pneumonia (CAP) have high short-term mortality, yet conventional severity scores do not incorporate bedside imaging or physiological frailty. In this study we aim to (1) evaluate the feasibility of obtaining lung ultrasound (LUS), quantitative chest computed tomography (CT), and Clinical Frailty Scale (CFS) assessments during the same admission and (2) explore the predictive potential for 28-day mortality by integrating imaging severity with physiological frailty.</p><p><strong>Methods: </strong>In this prospective, single-center pilot study (February 2022 - February 2025), we consecutively enrolled 60 hospitalized adults ≥ 65 years who met guideline criteria for severe CAP and completed 28-day follow-up. Twelve-zone LUS and CFS assessments were performed ≤ 24 h after admission; chest CT was acquired within 48 h when clinically permissible. Feasibility outcomes were recruitment rate, data completeness, and study-related adverse events. Associations with 28-day mortality were analyzed descriptively and with exploratory multivariable logistic regression.</p><p><strong>Results: </strong>LUS and CFS were completed in 100% and 93.3% of participants, respectively; CT was obtained in 83.3%. No study-related adverse events occurred. Twelve patients (20%) died within 28 days. Compared with survivors, non-survivors had higher median LUS scores (14.1 vs. 12.1), greater CT-defined consolidation (30% vs. 22% of lung volume), and a higher prevalence of severe frailty (58% vs. 25%). In the 50 participants with complete data, both LUS score (odds ratio [OR] 1.09 per point) and severe frailty (OR 3.85) independently predicted mortality. A model combining LUS and frailty improved discrimination relative to CURB-65 alone (area under the receiver-operating characteristic curve 0.75 vs. 0.68).</p><p><strong>Conclusions: </strong>Simultaneous acquisition of LUS, quantitative CT, and frailty metrics is feasible, safe, and well tolerated in elderly patients with severe CAP. Preliminary evidence suggests that integrating imaging severity with physiological frailty enhances short-term risk stratification beyond established clinical scores. These findings merit confirmation in larger, multicenter cohorts.</p>\",\"PeriodicalId\":9148,\"journal\":{\"name\":\"BMC Pulmonary Medicine\",\"volume\":\"25 1\",\"pages\":\"474\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-10-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12522310/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pulmonary Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12890-025-03950-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03950-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Predictive value of bedside lung ultrasound, quantitative chest CT, and frailty assessment for short-term outcomes in elderly patients with severe pneumonia: a pilot study.
Background: Elderly patients with severe community-acquired pneumonia (CAP) have high short-term mortality, yet conventional severity scores do not incorporate bedside imaging or physiological frailty. In this study we aim to (1) evaluate the feasibility of obtaining lung ultrasound (LUS), quantitative chest computed tomography (CT), and Clinical Frailty Scale (CFS) assessments during the same admission and (2) explore the predictive potential for 28-day mortality by integrating imaging severity with physiological frailty.
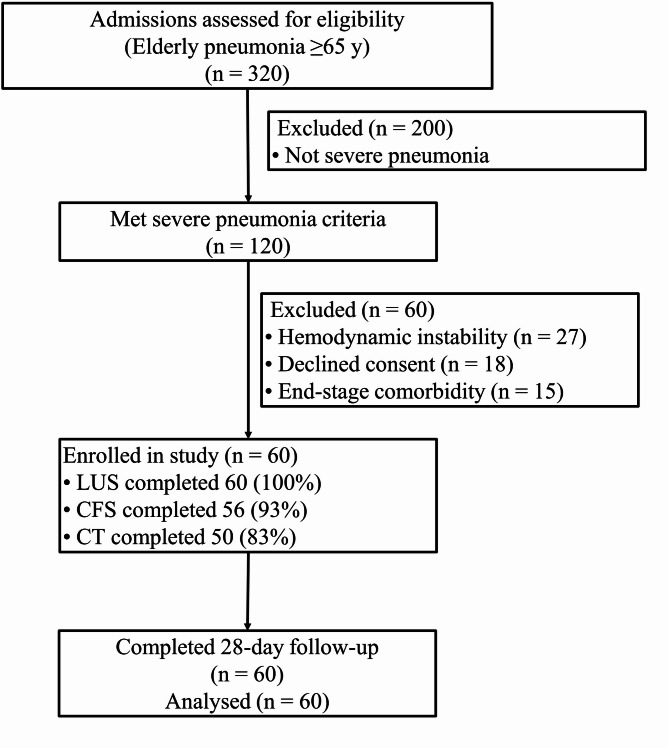
Methods: In this prospective, single-center pilot study (February 2022 - February 2025), we consecutively enrolled 60 hospitalized adults ≥ 65 years who met guideline criteria for severe CAP and completed 28-day follow-up. Twelve-zone LUS and CFS assessments were performed ≤ 24 h after admission; chest CT was acquired within 48 h when clinically permissible. Feasibility outcomes were recruitment rate, data completeness, and study-related adverse events. Associations with 28-day mortality were analyzed descriptively and with exploratory multivariable logistic regression.
Results: LUS and CFS were completed in 100% and 93.3% of participants, respectively; CT was obtained in 83.3%. No study-related adverse events occurred. Twelve patients (20%) died within 28 days. Compared with survivors, non-survivors had higher median LUS scores (14.1 vs. 12.1), greater CT-defined consolidation (30% vs. 22% of lung volume), and a higher prevalence of severe frailty (58% vs. 25%). In the 50 participants with complete data, both LUS score (odds ratio [OR] 1.09 per point) and severe frailty (OR 3.85) independently predicted mortality. A model combining LUS and frailty improved discrimination relative to CURB-65 alone (area under the receiver-operating characteristic curve 0.75 vs. 0.68).
Conclusions: Simultaneous acquisition of LUS, quantitative CT, and frailty metrics is feasible, safe, and well tolerated in elderly patients with severe CAP. Preliminary evidence suggests that integrating imaging severity with physiological frailty enhances short-term risk stratification beyond established clinical scores. These findings merit confirmation in larger, multicenter cohorts.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


