S D Robayo, C M Tansey, K Romanowski, J R Campbell
{"title":"移民中结核病的风险和后果及其预防的成本效用分析:系统回顾。","authors":"S D Robayo, C M Tansey, K Romanowski, J R Campbell","doi":"10.5588/ijtldopen.25.0355","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In low-TB incidence countries, foreign-born populations bear a disproportionate share of the TB burden. Cost-utility analyses of TB preventive treatment (TPT) programs among immigrants, however, have yielded divergent conclusions. We conducted a systematic review to evaluate how studies have considered the risks and consequences of TB disease and TPT.</p><p><strong>Methods: </strong>We searched PubMed and Embase for studies published from 1<sup>st</sup> January 2004 to 25<sup>th</sup> March 2025. We included modeling studies measuring health utility with quality-adjusted life years (QALYs) and evaluated TPT among immigrants to low TB incidence countries. Using a narrative synthesis, we examined how studies considered risks and consequences of TB disease and TPT and their impacts on health utility.</p><p><strong>Results: </strong>Of the 5,142 records screened, 14 studies met the inclusion criteria. Major adverse events (AEs) were the most frequently considered consequence of TPT with estimated risk ranging from 0% to 6% and mean associated annual disutility from major AEs was 0.017 QALYs, which varied substantially (coefficient of variation [CV)]: 1.2). All studies considered health disutility due to TB disease, with annual disutility ranging from 0.04 to 0.2 (mean: 0.11, CV: 0.4).</p><p><strong>Conclusions: </strong>There is wide variation in how risks and consequences of TPT and TB disease are considered in studies evaluating TB infection treatment programs.</p>","PeriodicalId":519984,"journal":{"name":"IJTLD open","volume":"2 10","pages":"555-562"},"PeriodicalIF":0.0000,"publicationDate":"2025-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12517258/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risks and consequences of TB and its prevention in cost-utility analyses among immigrants: a systematic review.\",\"authors\":\"S D Robayo, C M Tansey, K Romanowski, J R Campbell\",\"doi\":\"10.5588/ijtldopen.25.0355\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In low-TB incidence countries, foreign-born populations bear a disproportionate share of the TB burden. Cost-utility analyses of TB preventive treatment (TPT) programs among immigrants, however, have yielded divergent conclusions. We conducted a systematic review to evaluate how studies have considered the risks and consequences of TB disease and TPT.</p><p><strong>Methods: </strong>We searched PubMed and Embase for studies published from 1<sup>st</sup> January 2004 to 25<sup>th</sup> March 2025. We included modeling studies measuring health utility with quality-adjusted life years (QALYs) and evaluated TPT among immigrants to low TB incidence countries. Using a narrative synthesis, we examined how studies considered risks and consequences of TB disease and TPT and their impacts on health utility.</p><p><strong>Results: </strong>Of the 5,142 records screened, 14 studies met the inclusion criteria. Major adverse events (AEs) were the most frequently considered consequence of TPT with estimated risk ranging from 0% to 6% and mean associated annual disutility from major AEs was 0.017 QALYs, which varied substantially (coefficient of variation [CV)]: 1.2). All studies considered health disutility due to TB disease, with annual disutility ranging from 0.04 to 0.2 (mean: 0.11, CV: 0.4).</p><p><strong>Conclusions: </strong>There is wide variation in how risks and consequences of TPT and TB disease are considered in studies evaluating TB infection treatment programs.</p>\",\"PeriodicalId\":519984,\"journal\":{\"name\":\"IJTLD open\",\"volume\":\"2 10\",\"pages\":\"555-562\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12517258/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJTLD open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5588/ijtldopen.25.0355\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJTLD open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/ijtldopen.25.0355","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Risks and consequences of TB and its prevention in cost-utility analyses among immigrants: a systematic review.
Background: In low-TB incidence countries, foreign-born populations bear a disproportionate share of the TB burden. Cost-utility analyses of TB preventive treatment (TPT) programs among immigrants, however, have yielded divergent conclusions. We conducted a systematic review to evaluate how studies have considered the risks and consequences of TB disease and TPT.
Methods: We searched PubMed and Embase for studies published from 1st January 2004 to 25th March 2025. We included modeling studies measuring health utility with quality-adjusted life years (QALYs) and evaluated TPT among immigrants to low TB incidence countries. Using a narrative synthesis, we examined how studies considered risks and consequences of TB disease and TPT and their impacts on health utility.
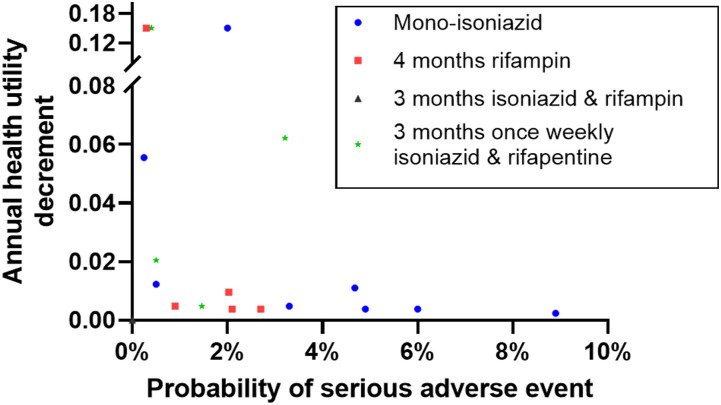
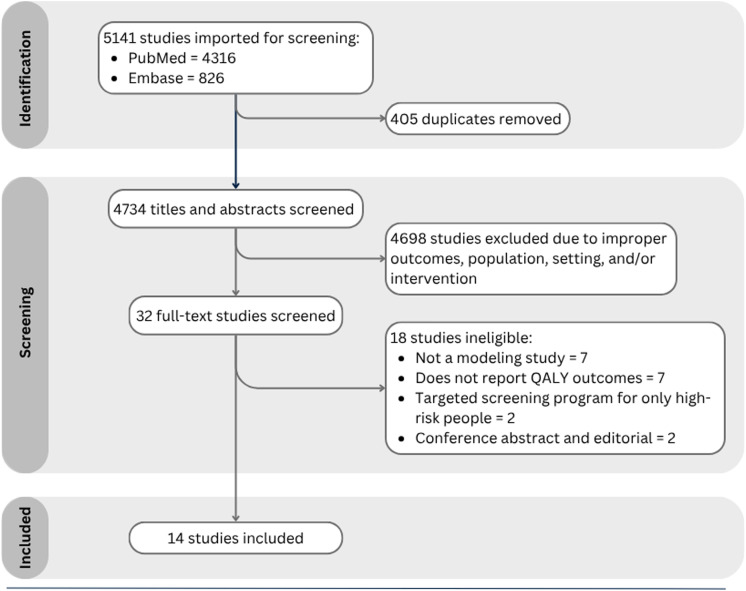
Results: Of the 5,142 records screened, 14 studies met the inclusion criteria. Major adverse events (AEs) were the most frequently considered consequence of TPT with estimated risk ranging from 0% to 6% and mean associated annual disutility from major AEs was 0.017 QALYs, which varied substantially (coefficient of variation [CV)]: 1.2). All studies considered health disutility due to TB disease, with annual disutility ranging from 0.04 to 0.2 (mean: 0.11, CV: 0.4).
Conclusions: There is wide variation in how risks and consequences of TPT and TB disease are considered in studies evaluating TB infection treatment programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


