David M Rub, Natalie Napolitano, Francis Simmons, Rachel Mackenzie, Kelle Matthews, Elizabeth E Foglia, Howard B Panitch
{"title":"使用电阻抗断层扫描评估临床指导的持续气道正压通气到稳定早产儿高流量鼻插管过渡:一项前瞻性观察研究。","authors":"David M Rub, Natalie Napolitano, Francis Simmons, Rachel Mackenzie, Kelle Matthews, Elizabeth E Foglia, Howard B Panitch","doi":"10.1002/ppul.71328","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess lung aeration changes during clinically directed transitions from CPAP to HFNC in preterm infants using Electrical Impedance Tomography (EIT).</p><p><strong>Design: </strong>Prospective, observational study.</p><p><strong>Setting: </strong>Single-center, Level IV Neonatal Intensive Care Unit.</p><p><strong>Patients: </strong>Infants born < 32 weeks gestational age (GA) undergoing a clinically indicated transition from CPAP to HFNC following ≥ 2 weeks of respiratory support.</p><p><strong>Interventions: </strong>EIT data were recorded for 30-60 min before and after transition.</p><p><strong>Main outcome measures: </strong>The primary outcome was change in end-expiratory lung impedance (ΔEELI). Infants were followed for 7 days following transition to assess for transition failure.</p><p><strong>Results: </strong>From 15 subjects, 4257 total breaths were analyzed. No significant difference in %∆EELI was found between HFNC and CPAP (Median ∆: -1.0%; IQR -3.6% to 6.0%; p = 0.78). The largest %∆EELI decrease (-9.8%) occurred in the subject who failed transition.</p><p><strong>Conclusions: </strong>Transitioning from CPAP to HFNC did not consistently decrease lung aeration in stable preterm infants. In the infant who failed transition, a distinct respiratory pattern was observed using EIT, characterized by a decrease in EELI and frequent recruitment breaths. These findings suggest better methods are needed to individualize and titrate respiratory support at the bedside for preterm infants.</p>","PeriodicalId":19932,"journal":{"name":"Pediatric Pulmonology","volume":"60 10","pages":"e71328"},"PeriodicalIF":2.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12522079/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating Clinically Directed Continuous Positive Airway Pressure to High Flow Nasal Cannula Transitions in Stable Preterm Infants Using Electrical Impedance Tomography: A Prospective, Observational Study.\",\"authors\":\"David M Rub, Natalie Napolitano, Francis Simmons, Rachel Mackenzie, Kelle Matthews, Elizabeth E Foglia, Howard B Panitch\",\"doi\":\"10.1002/ppul.71328\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To assess lung aeration changes during clinically directed transitions from CPAP to HFNC in preterm infants using Electrical Impedance Tomography (EIT).</p><p><strong>Design: </strong>Prospective, observational study.</p><p><strong>Setting: </strong>Single-center, Level IV Neonatal Intensive Care Unit.</p><p><strong>Patients: </strong>Infants born < 32 weeks gestational age (GA) undergoing a clinically indicated transition from CPAP to HFNC following ≥ 2 weeks of respiratory support.</p><p><strong>Interventions: </strong>EIT data were recorded for 30-60 min before and after transition.</p><p><strong>Main outcome measures: </strong>The primary outcome was change in end-expiratory lung impedance (ΔEELI). Infants were followed for 7 days following transition to assess for transition failure.</p><p><strong>Results: </strong>From 15 subjects, 4257 total breaths were analyzed. No significant difference in %∆EELI was found between HFNC and CPAP (Median ∆: -1.0%; IQR -3.6% to 6.0%; p = 0.78). The largest %∆EELI decrease (-9.8%) occurred in the subject who failed transition.</p><p><strong>Conclusions: </strong>Transitioning from CPAP to HFNC did not consistently decrease lung aeration in stable preterm infants. In the infant who failed transition, a distinct respiratory pattern was observed using EIT, characterized by a decrease in EELI and frequent recruitment breaths. These findings suggest better methods are needed to individualize and titrate respiratory support at the bedside for preterm infants.</p>\",\"PeriodicalId\":19932,\"journal\":{\"name\":\"Pediatric Pulmonology\",\"volume\":\"60 10\",\"pages\":\"e71328\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12522079/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Pulmonology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ppul.71328\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Pulmonology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ppul.71328","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:利用电阻抗断层扫描(EIT)评估早产儿从CPAP到HFNC临床过渡过程中肺通气量的变化。设计:前瞻性观察性研究。环境:单中心,四级新生儿重症监护病房。干预措施:记录转换前后30-60分钟的EIT数据。主要转归指标:主要转归指标为呼气末肺阻抗变化(ΔEELI)。婴儿在转换后随访7天以评估转换失败。结果:对15例患者进行了4257次全呼吸分析。HFNC与CPAP的%∆EELI无显著差异(中位数∆:-1.0%;IQR -3.6% ~ 6.0%; p = 0.78)。最大的∆EELI下降(-9.8%)发生在转换失败的受试者身上。结论:从CPAP过渡到HFNC并没有持续降低稳定早产儿的肺通气量。在转换失败的婴儿中,使用EIT观察到明显的呼吸模式,其特征是EELI减少和频繁的吸气呼吸。这些发现表明需要更好的方法来个性化和滴定早产儿床边的呼吸支持。
Evaluating Clinically Directed Continuous Positive Airway Pressure to High Flow Nasal Cannula Transitions in Stable Preterm Infants Using Electrical Impedance Tomography: A Prospective, Observational Study.
Objective: To assess lung aeration changes during clinically directed transitions from CPAP to HFNC in preterm infants using Electrical Impedance Tomography (EIT).
Design: Prospective, observational study.
Setting: Single-center, Level IV Neonatal Intensive Care Unit.
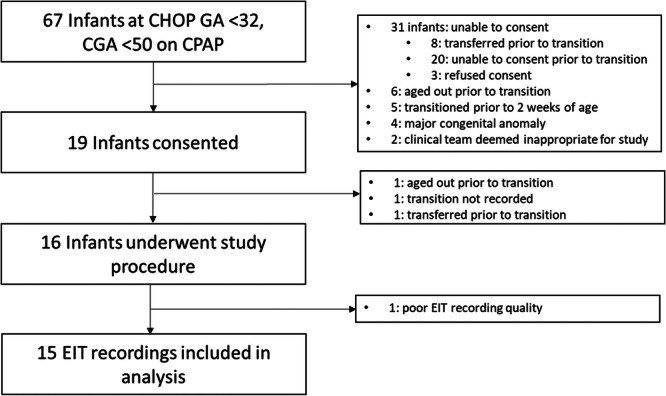
Patients: Infants born < 32 weeks gestational age (GA) undergoing a clinically indicated transition from CPAP to HFNC following ≥ 2 weeks of respiratory support.
Interventions: EIT data were recorded for 30-60 min before and after transition.
Main outcome measures: The primary outcome was change in end-expiratory lung impedance (ΔEELI). Infants were followed for 7 days following transition to assess for transition failure.
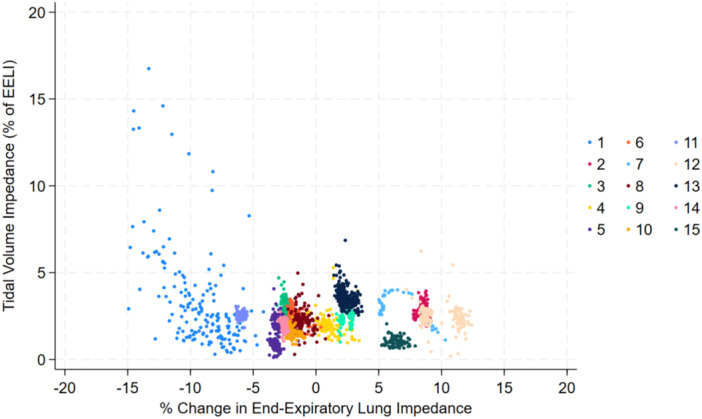
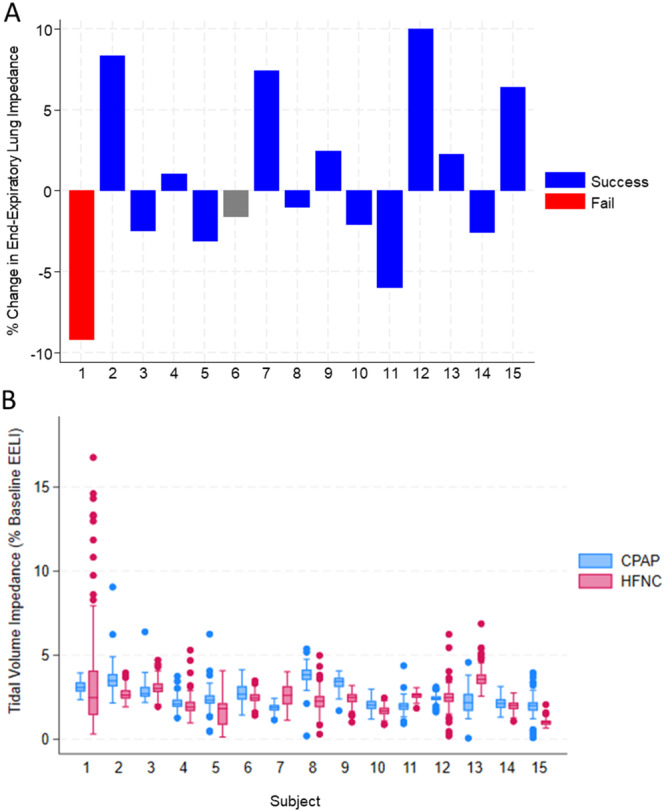
Results: From 15 subjects, 4257 total breaths were analyzed. No significant difference in %∆EELI was found between HFNC and CPAP (Median ∆: -1.0%; IQR -3.6% to 6.0%; p = 0.78). The largest %∆EELI decrease (-9.8%) occurred in the subject who failed transition.
Conclusions: Transitioning from CPAP to HFNC did not consistently decrease lung aeration in stable preterm infants. In the infant who failed transition, a distinct respiratory pattern was observed using EIT, characterized by a decrease in EELI and frequent recruitment breaths. These findings suggest better methods are needed to individualize and titrate respiratory support at the bedside for preterm infants.
期刊介绍:
Pediatric Pulmonology (PPUL) is the foremost global journal studying the respiratory system in disease and in health as it develops from intrauterine life though adolescence to adulthood. Combining explicit and informative analysis of clinical as well as basic scientific research, PPUL provides a look at the many facets of respiratory system disorders in infants and children, ranging from pathological anatomy, developmental issues, and pathophysiology to infectious disease, asthma, cystic fibrosis, and airborne toxins. Focused attention is given to the reporting of diagnostic and therapeutic methods for neonates, preschool children, and adolescents, the enduring effects of childhood respiratory diseases, and newly described infectious diseases.
PPUL concentrates on subject matters of crucial interest to specialists preparing for the Pediatric Subspecialty Examinations in the United States and other countries. With its attentive coverage and extensive clinical data, this journal is a principle source for pediatricians in practice and in training and a must have for all pediatric pulmonologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


