{"title":"当瞳孔说谎:揭露骨科手术中未被注意到的高位脊柱麻醉。","authors":"Kartik Sonawane, Sumeet Patil, Satheesh Kumar, Tuhin Mistry, Palanichamy Gurumoorthi, Chelliah Sekar","doi":"10.7759/cureus.94047","DOIUrl":null,"url":null,"abstract":"<p><p>High spinal anesthesia is a rare but potentially serious complication of neuraxial techniques. Unlike total spinal anesthesia, which typically presents dramatically with profound cardiovascular collapse, high spinal anesthesia may evolve more insidiously and manifest primarily with neurological signs. We report the case of a 23-year-old polytrauma patient undergoing femur and tibia fixation under combined spinal-epidural anesthesia (CSEA) who developed sudden unresponsiveness with fixed, dilated pupils shortly after femoral canal reaming. An epidural top-up of 10 mL 0.25% bupivacaine was administered 2.5 hours into surgery, with neurological deterioration occurring approximately 30 minutes later. Despite this alarming presentation, his hemodynamics and spontaneous ventilation remained stable, and he regained consciousness within 30 minutes without airway intervention. Postoperative evaluation revealed intrathecal migration of the epidural catheter, with the block extending above T2 and causing bilateral upper limb weakness. Arterial blood gas analysis demonstrated metabolic and respiratory acidosis, reflecting transient hypoventilation. This case illustrates how an unnoticed high spinal anesthesia can mimic catastrophic neurological or embolic events yet remain fully reversible. It underscores the importance of careful catheter management, structured differential diagnosis, and preparedness for airway intervention.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"17 10","pages":"e94047"},"PeriodicalIF":1.3000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12507387/pdf/","citationCount":"0","resultStr":"{\"title\":\"When the Pupils Lie: Unmasking an Unnoticed High Spinal Anesthesia During Orthopedic Surgery.\",\"authors\":\"Kartik Sonawane, Sumeet Patil, Satheesh Kumar, Tuhin Mistry, Palanichamy Gurumoorthi, Chelliah Sekar\",\"doi\":\"10.7759/cureus.94047\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>High spinal anesthesia is a rare but potentially serious complication of neuraxial techniques. Unlike total spinal anesthesia, which typically presents dramatically with profound cardiovascular collapse, high spinal anesthesia may evolve more insidiously and manifest primarily with neurological signs. We report the case of a 23-year-old polytrauma patient undergoing femur and tibia fixation under combined spinal-epidural anesthesia (CSEA) who developed sudden unresponsiveness with fixed, dilated pupils shortly after femoral canal reaming. An epidural top-up of 10 mL 0.25% bupivacaine was administered 2.5 hours into surgery, with neurological deterioration occurring approximately 30 minutes later. Despite this alarming presentation, his hemodynamics and spontaneous ventilation remained stable, and he regained consciousness within 30 minutes without airway intervention. Postoperative evaluation revealed intrathecal migration of the epidural catheter, with the block extending above T2 and causing bilateral upper limb weakness. Arterial blood gas analysis demonstrated metabolic and respiratory acidosis, reflecting transient hypoventilation. This case illustrates how an unnoticed high spinal anesthesia can mimic catastrophic neurological or embolic events yet remain fully reversible. It underscores the importance of careful catheter management, structured differential diagnosis, and preparedness for airway intervention.</p>\",\"PeriodicalId\":93960,\"journal\":{\"name\":\"Cureus\",\"volume\":\"17 10\",\"pages\":\"e94047\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-10-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12507387/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cureus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7759/cureus.94047\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.94047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
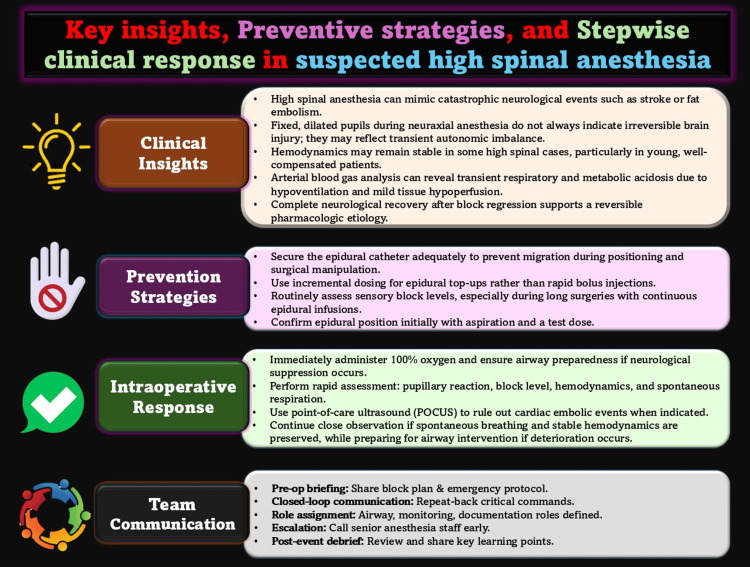
高位脊髓麻醉是一种罕见但潜在的严重并发症。与全脊髓麻醉不同,全脊髓麻醉通常表现为严重的心血管衰竭,高度脊髓麻醉可能更隐蔽地发展,主要表现为神经系统症状。我们报告一例23岁的多发性创伤患者,在脊髓-硬膜外联合麻醉(CSEA)下接受股骨和胫骨固定手术,在股骨管扩眼后不久,患者突然无反应,瞳孔固定扩大。手术2.5 小时后给予10 mL 0.25%布比卡因硬膜外补充,大约30 分钟后神经功能恶化。尽管有这种令人担忧的表现,他的血流动力学和自发通气仍然稳定,他在30 分钟内恢复了意识,没有气道干预。术后评估显示硬膜外导管鞘内移位,阻滞延伸至T2以上,导致双侧上肢无力。动脉血气分析显示代谢性和呼吸性酸中毒,反映短暂性低通气。这个病例说明了一个未被注意到的高位脊髓麻醉是如何模拟灾难性的神经或栓塞事件,但仍然是完全可逆的。它强调了仔细的导管管理,结构化的鉴别诊断和气道干预准备的重要性。
When the Pupils Lie: Unmasking an Unnoticed High Spinal Anesthesia During Orthopedic Surgery.
High spinal anesthesia is a rare but potentially serious complication of neuraxial techniques. Unlike total spinal anesthesia, which typically presents dramatically with profound cardiovascular collapse, high spinal anesthesia may evolve more insidiously and manifest primarily with neurological signs. We report the case of a 23-year-old polytrauma patient undergoing femur and tibia fixation under combined spinal-epidural anesthesia (CSEA) who developed sudden unresponsiveness with fixed, dilated pupils shortly after femoral canal reaming. An epidural top-up of 10 mL 0.25% bupivacaine was administered 2.5 hours into surgery, with neurological deterioration occurring approximately 30 minutes later. Despite this alarming presentation, his hemodynamics and spontaneous ventilation remained stable, and he regained consciousness within 30 minutes without airway intervention. Postoperative evaluation revealed intrathecal migration of the epidural catheter, with the block extending above T2 and causing bilateral upper limb weakness. Arterial blood gas analysis demonstrated metabolic and respiratory acidosis, reflecting transient hypoventilation. This case illustrates how an unnoticed high spinal anesthesia can mimic catastrophic neurological or embolic events yet remain fully reversible. It underscores the importance of careful catheter management, structured differential diagnosis, and preparedness for airway intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


