Andrea Llamas-Lopez, James A Seddon, Felicia C Chow, Caryn M Upton, Sanjay K Jain, Jan-Willem Alffenaar, Daniel J Grint, Kelly Dooley, Rob Aarnoutse, Fiona V Cresswell
{"title":"成人结核性脑膜炎的强化治疗:系统回顾和荟萃分析。","authors":"Andrea Llamas-Lopez, James A Seddon, Felicia C Chow, Caryn M Upton, Sanjay K Jain, Jan-Willem Alffenaar, Daniel J Grint, Kelly Dooley, Rob Aarnoutse, Fiona V Cresswell","doi":"10.1093/ofid/ofaf503","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tuberculous meningitis (TBM) remains the deadliest form of tuberculosis. Inadequate penetration of rifampicin and ethambutol into the brain and cerebrospinal fluid (CSF) may contribute to mortality. Over the last decade, research has focused on \"intensified\" treatment (higher-dose first-line drugs or addition of second-line drugs with good CSF penetration). This systematic review and meta-analysis evaluates the impact of intensified TBM treatment on mortality, disability, and safety.</p><p><strong>Methods: </strong>A systematic literature search was conducted of clinical trials examining intensified TBM treatments compared with a rifampicin-based standard-of-care regimen in adults. Odds ratios (ORs) were calculated using a random-effects model with mortality as the primary outcome, with OR <1 indicating lower mortality. Disability and safety were examined as secondary outcomes. Subgroup analyses included (1) higher-dose rifampicin, (2) addition of fluoroquinolones, and (3) addition of linezolid.</p><p><strong>Results: </strong>Ten trials meeting eligibility criteria, involving 1369 participants, were included. Higher-dose rifampicin (n = 1050; OR, 0.86; 95% CI, 0.54-1.35; <i>P</i> = .50), adjunctive fluoroquinolones (n = 1115; OR, 0.85; 95% CI, 0.56-1.27; <i>P</i> = .42), and linezolid (n = 79; OR, 0.73; 95% CI, 0.22-2.43; <i>P</i> = .61) did not significantly reduce TBM mortality. Due to heterogeneity in disability and safety endpoints, secondary outcomes could not be meta-analyzed.</p><p><strong>Conclusions: </strong>Current clinical trial evidence does not support the use of intensified TBM treatment in adults. However, these analyses are limited by diverse TBM case definitions, absence of MRC grading at enrollment, variable rifampicin dosing, limited data on linezolid and higher-dose isoniazid, and heterogeneous disability and safety outcomes. Use of uniform case definitions and consistent endpoints is essential to standardize data.</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 10","pages":"ofaf503"},"PeriodicalIF":3.8000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502660/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intensified Treatment of Tuberculous Meningitis in Adults: A Systematic Review and Meta-analysis.\",\"authors\":\"Andrea Llamas-Lopez, James A Seddon, Felicia C Chow, Caryn M Upton, Sanjay K Jain, Jan-Willem Alffenaar, Daniel J Grint, Kelly Dooley, Rob Aarnoutse, Fiona V Cresswell\",\"doi\":\"10.1093/ofid/ofaf503\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Tuberculous meningitis (TBM) remains the deadliest form of tuberculosis. Inadequate penetration of rifampicin and ethambutol into the brain and cerebrospinal fluid (CSF) may contribute to mortality. Over the last decade, research has focused on \\\"intensified\\\" treatment (higher-dose first-line drugs or addition of second-line drugs with good CSF penetration). This systematic review and meta-analysis evaluates the impact of intensified TBM treatment on mortality, disability, and safety.</p><p><strong>Methods: </strong>A systematic literature search was conducted of clinical trials examining intensified TBM treatments compared with a rifampicin-based standard-of-care regimen in adults. Odds ratios (ORs) were calculated using a random-effects model with mortality as the primary outcome, with OR <1 indicating lower mortality. Disability and safety were examined as secondary outcomes. Subgroup analyses included (1) higher-dose rifampicin, (2) addition of fluoroquinolones, and (3) addition of linezolid.</p><p><strong>Results: </strong>Ten trials meeting eligibility criteria, involving 1369 participants, were included. Higher-dose rifampicin (n = 1050; OR, 0.86; 95% CI, 0.54-1.35; <i>P</i> = .50), adjunctive fluoroquinolones (n = 1115; OR, 0.85; 95% CI, 0.56-1.27; <i>P</i> = .42), and linezolid (n = 79; OR, 0.73; 95% CI, 0.22-2.43; <i>P</i> = .61) did not significantly reduce TBM mortality. Due to heterogeneity in disability and safety endpoints, secondary outcomes could not be meta-analyzed.</p><p><strong>Conclusions: </strong>Current clinical trial evidence does not support the use of intensified TBM treatment in adults. However, these analyses are limited by diverse TBM case definitions, absence of MRC grading at enrollment, variable rifampicin dosing, limited data on linezolid and higher-dose isoniazid, and heterogeneous disability and safety outcomes. Use of uniform case definitions and consistent endpoints is essential to standardize data.</p>\",\"PeriodicalId\":19517,\"journal\":{\"name\":\"Open Forum Infectious Diseases\",\"volume\":\"12 10\",\"pages\":\"ofaf503\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-10-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502660/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Forum Infectious Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ofid/ofaf503\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofaf503","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Intensified Treatment of Tuberculous Meningitis in Adults: A Systematic Review and Meta-analysis.
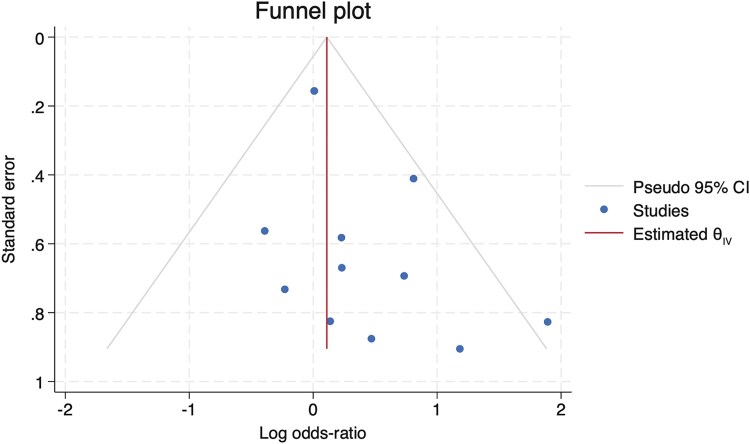
Background: Tuberculous meningitis (TBM) remains the deadliest form of tuberculosis. Inadequate penetration of rifampicin and ethambutol into the brain and cerebrospinal fluid (CSF) may contribute to mortality. Over the last decade, research has focused on "intensified" treatment (higher-dose first-line drugs or addition of second-line drugs with good CSF penetration). This systematic review and meta-analysis evaluates the impact of intensified TBM treatment on mortality, disability, and safety.
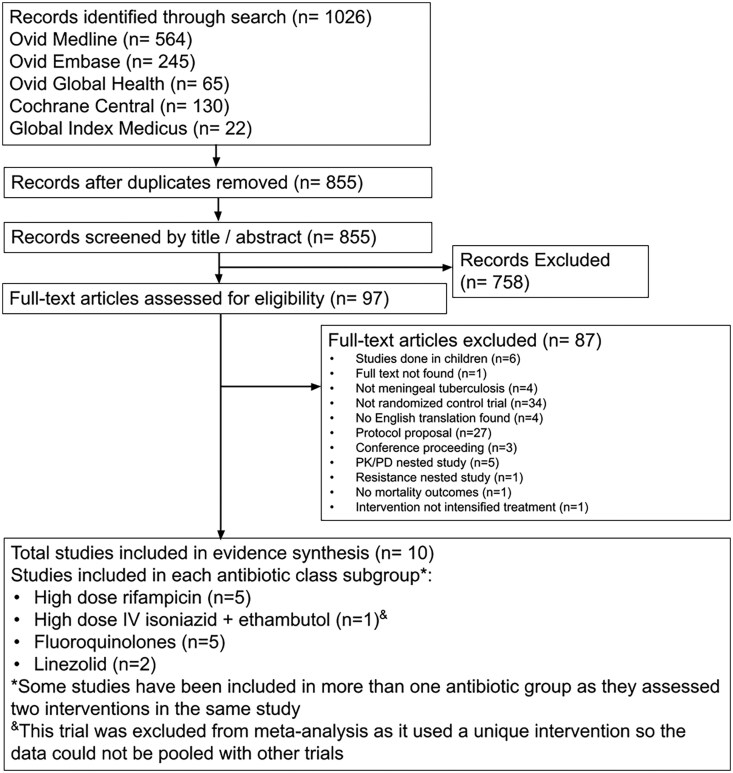
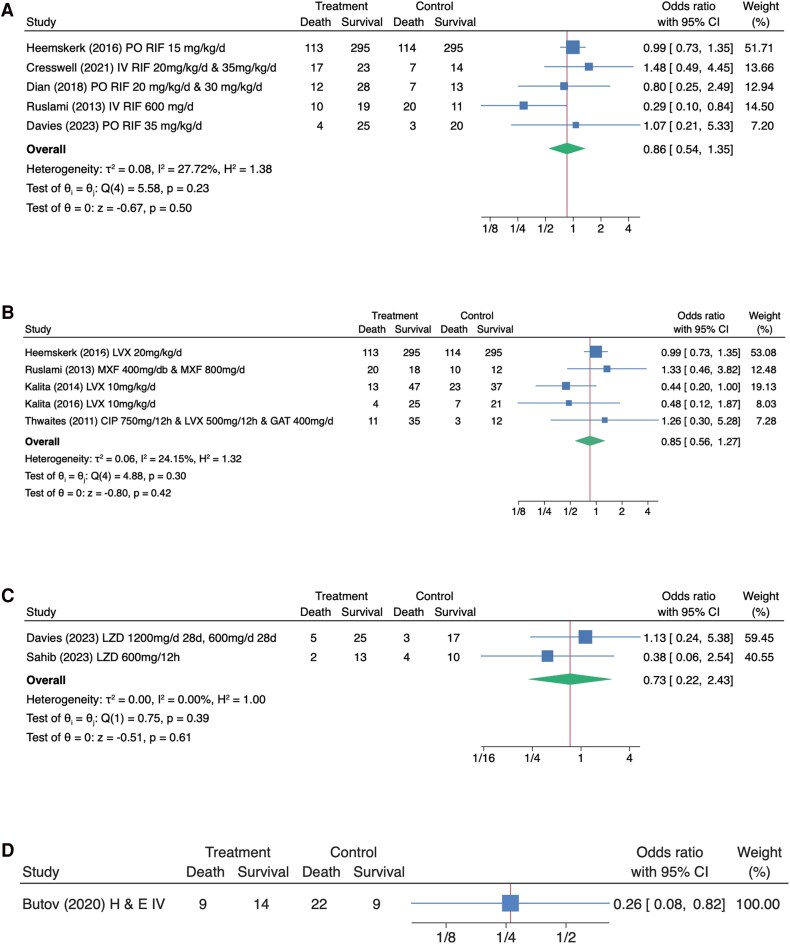
Methods: A systematic literature search was conducted of clinical trials examining intensified TBM treatments compared with a rifampicin-based standard-of-care regimen in adults. Odds ratios (ORs) were calculated using a random-effects model with mortality as the primary outcome, with OR <1 indicating lower mortality. Disability and safety were examined as secondary outcomes. Subgroup analyses included (1) higher-dose rifampicin, (2) addition of fluoroquinolones, and (3) addition of linezolid.
Results: Ten trials meeting eligibility criteria, involving 1369 participants, were included. Higher-dose rifampicin (n = 1050; OR, 0.86; 95% CI, 0.54-1.35; P = .50), adjunctive fluoroquinolones (n = 1115; OR, 0.85; 95% CI, 0.56-1.27; P = .42), and linezolid (n = 79; OR, 0.73; 95% CI, 0.22-2.43; P = .61) did not significantly reduce TBM mortality. Due to heterogeneity in disability and safety endpoints, secondary outcomes could not be meta-analyzed.
Conclusions: Current clinical trial evidence does not support the use of intensified TBM treatment in adults. However, these analyses are limited by diverse TBM case definitions, absence of MRC grading at enrollment, variable rifampicin dosing, limited data on linezolid and higher-dose isoniazid, and heterogeneous disability and safety outcomes. Use of uniform case definitions and consistent endpoints is essential to standardize data.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


