Hui Lian, Guangjian Wang, Qing Zhang, Hua Zhao, Xiaoting Wang
{"title":"一项前瞻性研究:ICU老年患者的年龄分层免疫炎症特征和预后意义。","authors":"Hui Lian, Guangjian Wang, Qing Zhang, Hua Zhao, Xiaoting Wang","doi":"10.2147/JIR.S548582","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aging population has advanced older patients (OPs) in intensive care units (ICUs). Critical illness and aging exacerbate immune-inflammatory dysregulation, impairing immune interactions and worsening prognosis. However, knowledge regarding immune-inflammatory profiles and prognostic implications for OPs, particularly in very old patients (VOPs), remains limited.</p><p><strong>Methods: </strong>This single-center prospective study included patients aged ≥65 with hemodynamically confirmed shock, signifying severe critical illness admitted between August 2023 and February 2025. Demographic, medication, and laboratory data were collected from electronic medical records. The primary endpoint was in-hospital mortality; secondary endpoints included ICU and hospital stay duration. Participants aged 65-74 were young old patients (YOPs), and those aged ≥75 as VOPs. Statistical analysis included χ² for categorical variables, Kolmogorov-Smirnov for non-normal continuous data, Principal component analysis (PCA) for inflammatory states, while generalized additive mixed models for statistical interactions.</p><p><strong>Results: </strong>A total of 537 OPs were admitted, with no significant differences in inflammatory markers between YOPs and VOPs, except fibrinogen. Survivors had higher levels of hypersensitive C-reactive protein (hsCRP). Lymphocyte counts and subtypes were reduced in OPs. VOPs showed higher natural killer cells, CD8+CD38+, and CD8+DR+ counts versus YOPs. The median CD8+DR+ count was 82 in survivors versus 59 in non-survivors. Among VOPs, hsCRP, interleukin-8, and immunoglobulin G showed significant differences. B cell count was lower (median 104 vs 72), and CD8+ T cell activation declined in non-survivors. Mortality was higher in the low inflammatory state group. As B and T cell counts increased, mortality decreased in high inflammatory states. Higher CD8+DR+ counts reduced mortality.</p><p><strong>Conclusion: </strong>OPs, especially VOPs, with hemodynamically confirmed shock and critical illness exhibit distinct immune-inflammatory characteristics affecting prognosis. A weakened immune response in low inflammation links to poor outcomes. Enhancing B cell and CD8+DR+ T cell responses may improve prognosis through precise immune regulation in ICU settings.</p>","PeriodicalId":16107,"journal":{"name":"Journal of Inflammation Research","volume":"18 ","pages":"13727-13743"},"PeriodicalIF":4.1000,"publicationDate":"2025-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502966/pdf/","citationCount":"0","resultStr":"{\"title\":\"Age-Stratified Immune-Inflammatory Profiles and Prognostic Implications of Old Patients in the ICU: A Prospective Study.\",\"authors\":\"Hui Lian, Guangjian Wang, Qing Zhang, Hua Zhao, Xiaoting Wang\",\"doi\":\"10.2147/JIR.S548582\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aging population has advanced older patients (OPs) in intensive care units (ICUs). Critical illness and aging exacerbate immune-inflammatory dysregulation, impairing immune interactions and worsening prognosis. However, knowledge regarding immune-inflammatory profiles and prognostic implications for OPs, particularly in very old patients (VOPs), remains limited.</p><p><strong>Methods: </strong>This single-center prospective study included patients aged ≥65 with hemodynamically confirmed shock, signifying severe critical illness admitted between August 2023 and February 2025. Demographic, medication, and laboratory data were collected from electronic medical records. The primary endpoint was in-hospital mortality; secondary endpoints included ICU and hospital stay duration. Participants aged 65-74 were young old patients (YOPs), and those aged ≥75 as VOPs. Statistical analysis included χ² for categorical variables, Kolmogorov-Smirnov for non-normal continuous data, Principal component analysis (PCA) for inflammatory states, while generalized additive mixed models for statistical interactions.</p><p><strong>Results: </strong>A total of 537 OPs were admitted, with no significant differences in inflammatory markers between YOPs and VOPs, except fibrinogen. Survivors had higher levels of hypersensitive C-reactive protein (hsCRP). Lymphocyte counts and subtypes were reduced in OPs. VOPs showed higher natural killer cells, CD8+CD38+, and CD8+DR+ counts versus YOPs. The median CD8+DR+ count was 82 in survivors versus 59 in non-survivors. Among VOPs, hsCRP, interleukin-8, and immunoglobulin G showed significant differences. B cell count was lower (median 104 vs 72), and CD8+ T cell activation declined in non-survivors. Mortality was higher in the low inflammatory state group. As B and T cell counts increased, mortality decreased in high inflammatory states. Higher CD8+DR+ counts reduced mortality.</p><p><strong>Conclusion: </strong>OPs, especially VOPs, with hemodynamically confirmed shock and critical illness exhibit distinct immune-inflammatory characteristics affecting prognosis. A weakened immune response in low inflammation links to poor outcomes. Enhancing B cell and CD8+DR+ T cell responses may improve prognosis through precise immune regulation in ICU settings.</p>\",\"PeriodicalId\":16107,\"journal\":{\"name\":\"Journal of Inflammation Research\",\"volume\":\"18 \",\"pages\":\"13727-13743\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2025-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502966/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Inflammation Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/JIR.S548582\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Inflammation Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JIR.S548582","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:人口老龄化导致重症监护病房(icu)出现高龄患者(OPs)。危重疾病和衰老加剧免疫炎症失调,损害免疫相互作用,恶化预后。然而,关于免疫炎症特征和OPs的预后影响的知识,特别是在非常老的患者(VOPs)中,仍然有限。方法:这项单中心前瞻性研究纳入了2023年8月至2025年2月期间入院的年龄≥65岁、经血流动力学证实为休克的重症患者。从电子病历中收集人口统计、药物和实验室数据。主要终点是住院死亡率;次要终点包括ICU和住院时间。65-74岁为年轻老年患者(YOPs),≥75岁为VOPs。统计分析包括分类变量的χ 2,非正态连续数据的Kolmogorov-Smirnov,炎症状态的主成分分析(PCA),以及统计相互作用的广义加性混合模型。结果:共入院537例OPs,除纤维蛋白原外,YOPs与VOPs之间的炎症标志物无显著差异。幸存者有更高水平的超敏c反应蛋白(hsCRP)。淋巴细胞计数和亚型减少。与YOPs相比,VOPs显示更高的自然杀伤细胞、CD8+CD38+和CD8+DR+计数。幸存者的中位CD8+DR+计数为82,非幸存者为59。在VOPs中,hsCRP、白细胞介素-8、免疫球蛋白G有显著性差异。B细胞计数较低(中位104 vs 72),非幸存者的CD8+ T细胞活化下降。低炎症状态组死亡率较高。随着B细胞和T细胞计数的增加,高炎症状态下的死亡率降低。较高的CD8+DR+计数降低了死亡率。结论:血液动力学证实的休克和危重疾病的OPs,尤其是VOPs,具有明显的免疫炎症特征,影响预后。低炎症的免疫反应减弱与预后不良有关。加强B细胞和CD8+DR+ T细胞反应可能通过精确的免疫调节改善ICU患者的预后。
Age-Stratified Immune-Inflammatory Profiles and Prognostic Implications of Old Patients in the ICU: A Prospective Study.
Background: The aging population has advanced older patients (OPs) in intensive care units (ICUs). Critical illness and aging exacerbate immune-inflammatory dysregulation, impairing immune interactions and worsening prognosis. However, knowledge regarding immune-inflammatory profiles and prognostic implications for OPs, particularly in very old patients (VOPs), remains limited.
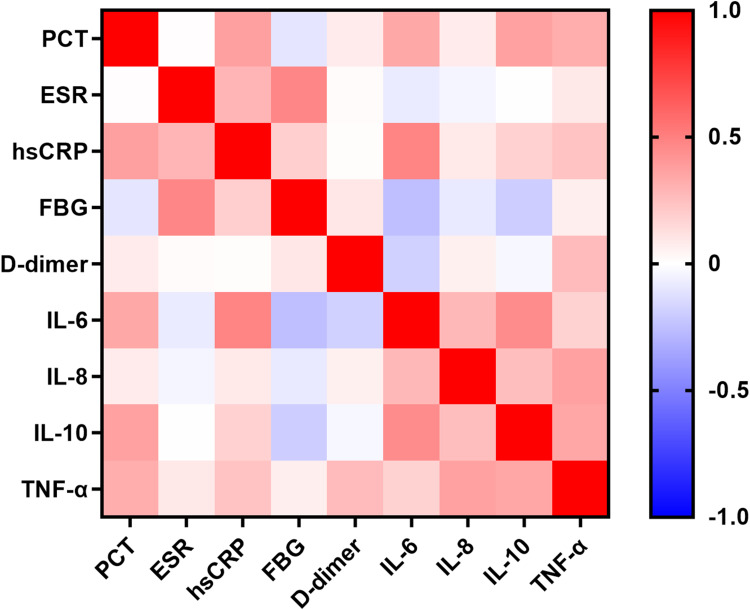
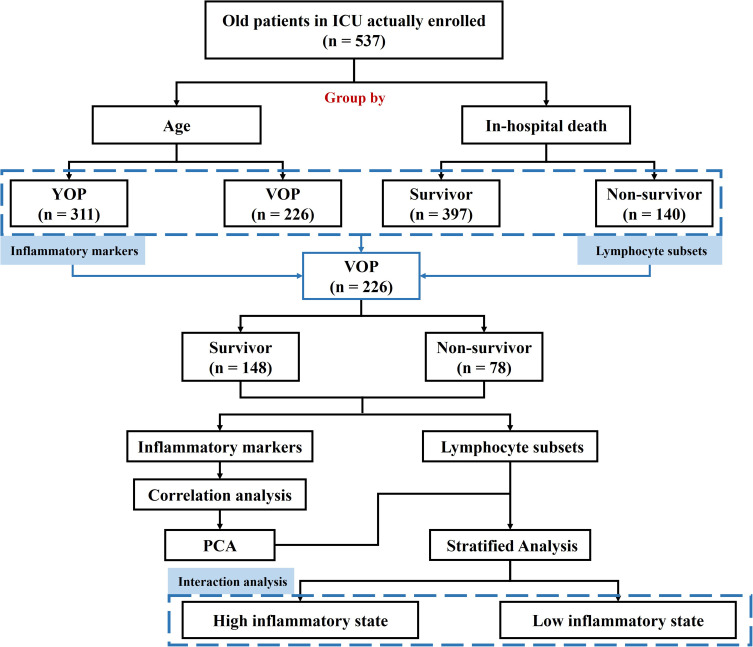
Methods: This single-center prospective study included patients aged ≥65 with hemodynamically confirmed shock, signifying severe critical illness admitted between August 2023 and February 2025. Demographic, medication, and laboratory data were collected from electronic medical records. The primary endpoint was in-hospital mortality; secondary endpoints included ICU and hospital stay duration. Participants aged 65-74 were young old patients (YOPs), and those aged ≥75 as VOPs. Statistical analysis included χ² for categorical variables, Kolmogorov-Smirnov for non-normal continuous data, Principal component analysis (PCA) for inflammatory states, while generalized additive mixed models for statistical interactions.
Results: A total of 537 OPs were admitted, with no significant differences in inflammatory markers between YOPs and VOPs, except fibrinogen. Survivors had higher levels of hypersensitive C-reactive protein (hsCRP). Lymphocyte counts and subtypes were reduced in OPs. VOPs showed higher natural killer cells, CD8+CD38+, and CD8+DR+ counts versus YOPs. The median CD8+DR+ count was 82 in survivors versus 59 in non-survivors. Among VOPs, hsCRP, interleukin-8, and immunoglobulin G showed significant differences. B cell count was lower (median 104 vs 72), and CD8+ T cell activation declined in non-survivors. Mortality was higher in the low inflammatory state group. As B and T cell counts increased, mortality decreased in high inflammatory states. Higher CD8+DR+ counts reduced mortality.
Conclusion: OPs, especially VOPs, with hemodynamically confirmed shock and critical illness exhibit distinct immune-inflammatory characteristics affecting prognosis. A weakened immune response in low inflammation links to poor outcomes. Enhancing B cell and CD8+DR+ T cell responses may improve prognosis through precise immune regulation in ICU settings.
期刊介绍:
An international, peer-reviewed, open access, online journal that welcomes laboratory and clinical findings on the molecular basis, cell biology and pharmacology of inflammation.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


