Cuie Chen, Yuechong Cui, Shujun Chen, Jiaonv Chen, Lirong Zhao, Yuanyuan Sun, Liuqing Ji, Guoliang Wang
{"title":"超声心动图与全身血流动力学参数的结合对早产儿血流动力学意义显著的动脉导管未闭的早期危险分层。","authors":"Cuie Chen, Yuechong Cui, Shujun Chen, Jiaonv Chen, Lirong Zhao, Yuanyuan Sun, Liuqing Ji, Guoliang Wang","doi":"10.3389/fped.2025.1616706","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hemodynamically significant patent ductus arteriosus (hsPDA) is a major contributor to morbidity and mortality in extremely preterm infants. Both echocardiographic assessment and systemic hemodynamic monitoring have emerged as valuable tools for evaluating cardiovascular status during the early postnatal period. This study aimed to evaluate whether echocardiographic and systemic hemodynamic parameters within 72 hours can predict the development of hsPDA in preterm infants.</p><p><strong>Methods: </strong>In this prospective study, 98 infants born at our institution between October 2022 and March 2025 were enrolled based on inclusion criteria of gestational age ≤32 weeks and birth weight ≤1,500 g. Hemodynamic monitoring was conducted using the Non-Invasive Cardiac System (NICaS) at 24, 48, and 72 hours after birth, each followed immediately by echocardiographic evaluation.</p><p><strong>Results: </strong>Among 98 preterm infants, 85 had patent ductus arteriosus (PDA) at 24 hours, with 30 progressing to hsPDA. The hsPDA group had significantly lower gestational age and birth weight. Maternal eclampsia or preeclampsia, placental abruption, neonatal asphyxia, alveolar surfactant need, mechanical ventilation within 72 hours, and higher fluid intake in the first 24 hours were more frequent in this group. These infants required prolonged respiratory support and parenteral nutrition, and showed higher rates of intraventricular hemorrhage (IVH) and bronchopulmonary dysplasia (BPD). Compared to non-hsPDA infants, those with hsPDA had larger ductus arteriosus (DA) diameters, higher DA diameter/weight ratios at 48 and 72 hours, and elevated left atrium-to-aortic root (LA/Ao) ratios at 24, 48, and 72 hours. Stroke index (SI), cardiac output index (CI), and total body water percent (TBW%) were increased, while total peripheral resistance index (TPRI) was reduced at 48 and 72 hours. Multivariate analysis identified maternal eclampsia/preeclampsia, surfactant use, DA diameter-to-weight ratio, LA/Ao, and TBW% at 48 and 72 hours as independent risk factors. A combined model achieved high predictive accuracy (AUC = 0.981, sensitivity = 100%, specificity = 90.0%).</p><p><strong>Conclusion: </strong>This study demonstrated that combining echocardiographic parameters with systemic hemodynamic indicators at 72 hours of life provides significant predictive value for identifying preterm infants with a gestational age ≤32 weeks and birth weight ≤1,500 g who are at risk of developing hsPDA.</p>","PeriodicalId":12637,"journal":{"name":"Frontiers in Pediatrics","volume":"13 ","pages":"1616706"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502083/pdf/","citationCount":"0","resultStr":"{\"title\":\"Combination of echocardiography with systemic hemodynamic parameters for early risk stratification of hemodynamically significant patent ductus arteriosus in preterm infants.\",\"authors\":\"Cuie Chen, Yuechong Cui, Shujun Chen, Jiaonv Chen, Lirong Zhao, Yuanyuan Sun, Liuqing Ji, Guoliang Wang\",\"doi\":\"10.3389/fped.2025.1616706\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hemodynamically significant patent ductus arteriosus (hsPDA) is a major contributor to morbidity and mortality in extremely preterm infants. Both echocardiographic assessment and systemic hemodynamic monitoring have emerged as valuable tools for evaluating cardiovascular status during the early postnatal period. This study aimed to evaluate whether echocardiographic and systemic hemodynamic parameters within 72 hours can predict the development of hsPDA in preterm infants.</p><p><strong>Methods: </strong>In this prospective study, 98 infants born at our institution between October 2022 and March 2025 were enrolled based on inclusion criteria of gestational age ≤32 weeks and birth weight ≤1,500 g. Hemodynamic monitoring was conducted using the Non-Invasive Cardiac System (NICaS) at 24, 48, and 72 hours after birth, each followed immediately by echocardiographic evaluation.</p><p><strong>Results: </strong>Among 98 preterm infants, 85 had patent ductus arteriosus (PDA) at 24 hours, with 30 progressing to hsPDA. The hsPDA group had significantly lower gestational age and birth weight. Maternal eclampsia or preeclampsia, placental abruption, neonatal asphyxia, alveolar surfactant need, mechanical ventilation within 72 hours, and higher fluid intake in the first 24 hours were more frequent in this group. These infants required prolonged respiratory support and parenteral nutrition, and showed higher rates of intraventricular hemorrhage (IVH) and bronchopulmonary dysplasia (BPD). Compared to non-hsPDA infants, those with hsPDA had larger ductus arteriosus (DA) diameters, higher DA diameter/weight ratios at 48 and 72 hours, and elevated left atrium-to-aortic root (LA/Ao) ratios at 24, 48, and 72 hours. Stroke index (SI), cardiac output index (CI), and total body water percent (TBW%) were increased, while total peripheral resistance index (TPRI) was reduced at 48 and 72 hours. Multivariate analysis identified maternal eclampsia/preeclampsia, surfactant use, DA diameter-to-weight ratio, LA/Ao, and TBW% at 48 and 72 hours as independent risk factors. A combined model achieved high predictive accuracy (AUC = 0.981, sensitivity = 100%, specificity = 90.0%).</p><p><strong>Conclusion: </strong>This study demonstrated that combining echocardiographic parameters with systemic hemodynamic indicators at 72 hours of life provides significant predictive value for identifying preterm infants with a gestational age ≤32 weeks and birth weight ≤1,500 g who are at risk of developing hsPDA.</p>\",\"PeriodicalId\":12637,\"journal\":{\"name\":\"Frontiers in Pediatrics\",\"volume\":\"13 \",\"pages\":\"1616706\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502083/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fped.2025.1616706\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fped.2025.1616706","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Combination of echocardiography with systemic hemodynamic parameters for early risk stratification of hemodynamically significant patent ductus arteriosus in preterm infants.
Background: Hemodynamically significant patent ductus arteriosus (hsPDA) is a major contributor to morbidity and mortality in extremely preterm infants. Both echocardiographic assessment and systemic hemodynamic monitoring have emerged as valuable tools for evaluating cardiovascular status during the early postnatal period. This study aimed to evaluate whether echocardiographic and systemic hemodynamic parameters within 72 hours can predict the development of hsPDA in preterm infants.
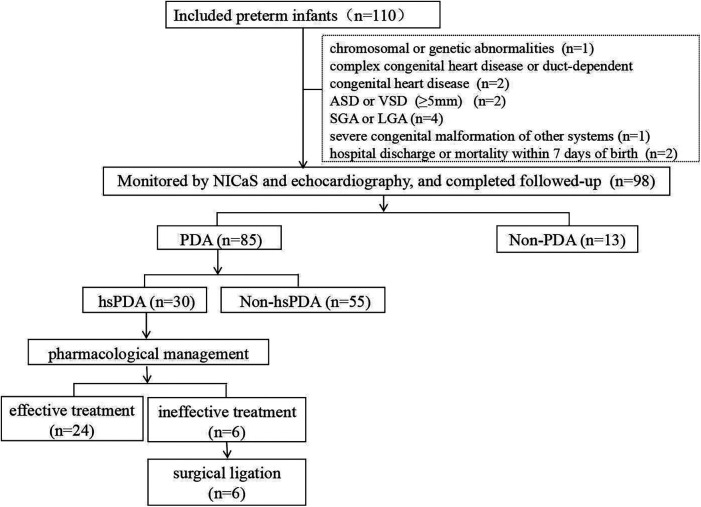
Methods: In this prospective study, 98 infants born at our institution between October 2022 and March 2025 were enrolled based on inclusion criteria of gestational age ≤32 weeks and birth weight ≤1,500 g. Hemodynamic monitoring was conducted using the Non-Invasive Cardiac System (NICaS) at 24, 48, and 72 hours after birth, each followed immediately by echocardiographic evaluation.
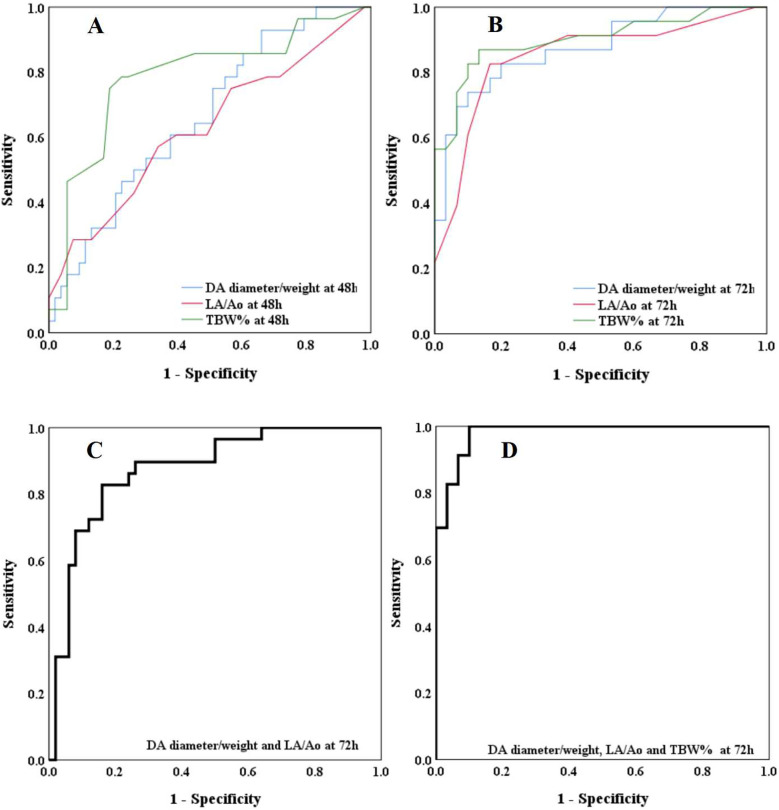
Results: Among 98 preterm infants, 85 had patent ductus arteriosus (PDA) at 24 hours, with 30 progressing to hsPDA. The hsPDA group had significantly lower gestational age and birth weight. Maternal eclampsia or preeclampsia, placental abruption, neonatal asphyxia, alveolar surfactant need, mechanical ventilation within 72 hours, and higher fluid intake in the first 24 hours were more frequent in this group. These infants required prolonged respiratory support and parenteral nutrition, and showed higher rates of intraventricular hemorrhage (IVH) and bronchopulmonary dysplasia (BPD). Compared to non-hsPDA infants, those with hsPDA had larger ductus arteriosus (DA) diameters, higher DA diameter/weight ratios at 48 and 72 hours, and elevated left atrium-to-aortic root (LA/Ao) ratios at 24, 48, and 72 hours. Stroke index (SI), cardiac output index (CI), and total body water percent (TBW%) were increased, while total peripheral resistance index (TPRI) was reduced at 48 and 72 hours. Multivariate analysis identified maternal eclampsia/preeclampsia, surfactant use, DA diameter-to-weight ratio, LA/Ao, and TBW% at 48 and 72 hours as independent risk factors. A combined model achieved high predictive accuracy (AUC = 0.981, sensitivity = 100%, specificity = 90.0%).
Conclusion: This study demonstrated that combining echocardiographic parameters with systemic hemodynamic indicators at 72 hours of life provides significant predictive value for identifying preterm infants with a gestational age ≤32 weeks and birth weight ≤1,500 g who are at risk of developing hsPDA.
期刊介绍:
Frontiers in Pediatrics (Impact Factor 2.33) publishes rigorously peer-reviewed research broadly across the field, from basic to clinical research that meets ongoing challenges in pediatric patient care and child health. Field Chief Editors Arjan Te Pas at Leiden University and Michael L. Moritz at the Children''s Hospital of Pittsburgh are supported by an outstanding Editorial Board of international experts. This multidisciplinary open-access journal is at the forefront of disseminating and communicating scientific knowledge and impactful discoveries to researchers, academics, clinicians and the public worldwide.
Frontiers in Pediatrics also features Research Topics, Frontiers special theme-focused issues managed by Guest Associate Editors, addressing important areas in pediatrics. In this fashion, Frontiers serves as an outlet to publish the broadest aspects of pediatrics in both basic and clinical research, including high-quality reviews, case reports, editorials and commentaries related to all aspects of pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


