{"title":"无严重三尖瓣反流的急性心力衰竭患者肺动脉收缩压阈值定义肺和外周充血。","authors":"Maria Giulia Bellicini","doi":"10.3389/fcvm.2025.1678712","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Pulmonary and/or peripheral venous congestion defines the clinical diagnosis of acute heart failure (AHF). However, the systolic pulmonary arterial pressure (sPAP) thresholds at which pulmonary (chest x-ray) and inferior vena cava (IVC) congestion occur are not well established. This study aimed to identify a cut-off value of sPAP that reliably indicates AHF.</p><p><strong>Methods and results: </strong>We retrospectively included 380 consecutive patients hospitalized for AHF at an Italian referral centre, after excluding those with severe tricuspid regurgitation. Receiver operating characteristic (ROC) curve analysis and Youden's J statistic identified a threshold of sPAP ≥ 48.75 mmHg as the most accurate in predicting both pulmonary (sensitivity = 89.9%, specificity = 73%) and peripheral (sensitivity = 88.3%, specificity = 82.5%) fluid overload. The association between this sPAP threshold and both pulmonary and peripheral congestion was confirmed by chi-square testing (<i>p</i> < 0.001) and multivariate logistic regression (<i>p</i> < 0.001). After adjustment for confounders, sPAP ≥ 49 mmHg was independently associated with all-cause death or heart failure (HF) hospitalization (HR = 1.713; 95% CI 1.127-2.602; <i>p</i> = 0.012).</p><p><strong>Conclusions: </strong>sPAP threshold of 49 mmHg identifies congestion with clinically useful accuracy-pulmonary (chest X-ray) congestion.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1678712"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500580/pdf/","citationCount":"0","resultStr":"{\"title\":\"Systolic pulmonary artery pressure threshold to define pulmonary and peripheral congestion in acute heart failure in absence of severe tricuspid regurgitation.\",\"authors\":\"Maria Giulia Bellicini\",\"doi\":\"10.3389/fcvm.2025.1678712\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aims: </strong>Pulmonary and/or peripheral venous congestion defines the clinical diagnosis of acute heart failure (AHF). However, the systolic pulmonary arterial pressure (sPAP) thresholds at which pulmonary (chest x-ray) and inferior vena cava (IVC) congestion occur are not well established. This study aimed to identify a cut-off value of sPAP that reliably indicates AHF.</p><p><strong>Methods and results: </strong>We retrospectively included 380 consecutive patients hospitalized for AHF at an Italian referral centre, after excluding those with severe tricuspid regurgitation. Receiver operating characteristic (ROC) curve analysis and Youden's J statistic identified a threshold of sPAP ≥ 48.75 mmHg as the most accurate in predicting both pulmonary (sensitivity = 89.9%, specificity = 73%) and peripheral (sensitivity = 88.3%, specificity = 82.5%) fluid overload. The association between this sPAP threshold and both pulmonary and peripheral congestion was confirmed by chi-square testing (<i>p</i> < 0.001) and multivariate logistic regression (<i>p</i> < 0.001). After adjustment for confounders, sPAP ≥ 49 mmHg was independently associated with all-cause death or heart failure (HF) hospitalization (HR = 1.713; 95% CI 1.127-2.602; <i>p</i> = 0.012).</p><p><strong>Conclusions: </strong>sPAP threshold of 49 mmHg identifies congestion with clinically useful accuracy-pulmonary (chest X-ray) congestion.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1678712\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500580/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1678712\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1678712","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
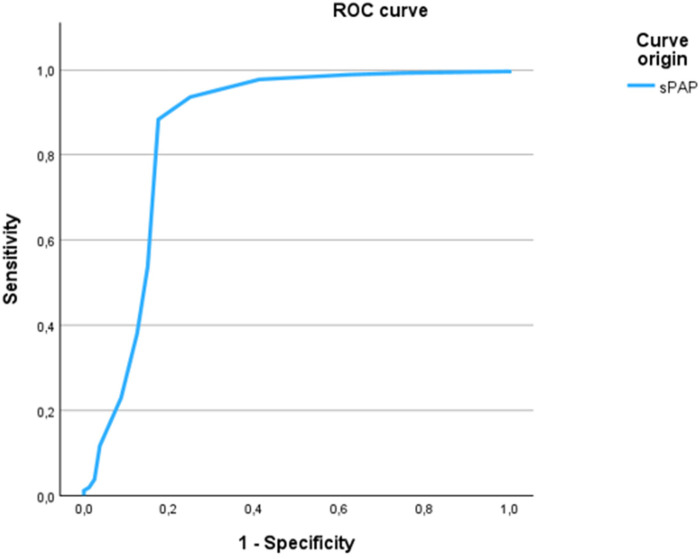
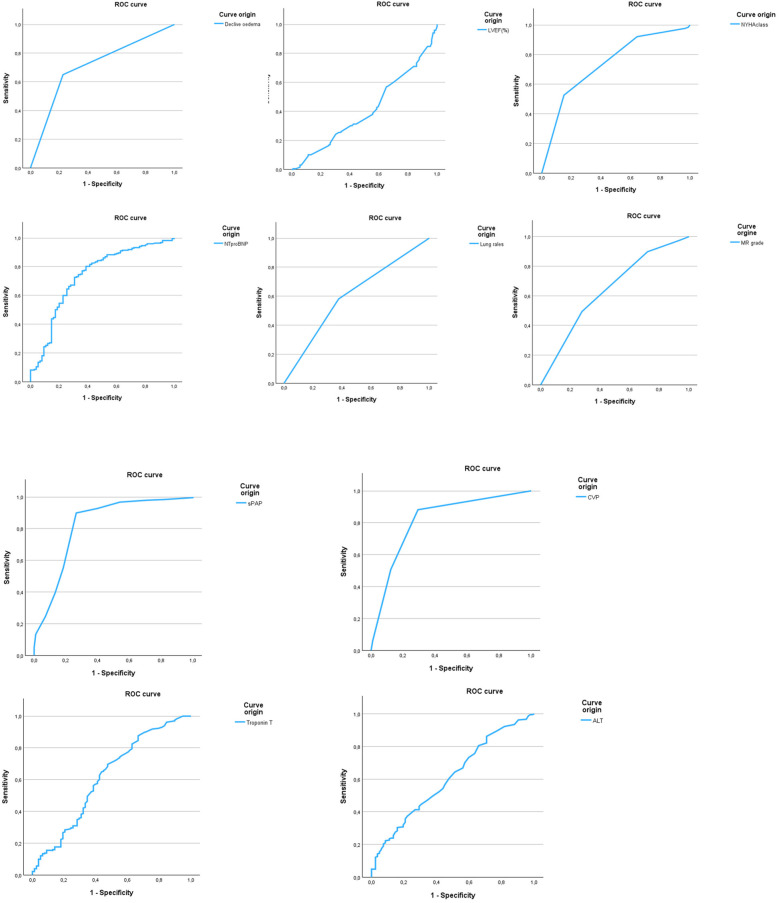
背景和目的:肺和/或周围静脉充血定义急性心力衰竭(AHF)的临床诊断。然而,肺(胸部x线)和下腔静脉(IVC)充血发生的收缩期肺动脉压(sPAP)阈值尚未得到很好的确定。本研究旨在确定sPAP的截断值,该截断值可靠地指示AHF。方法和结果:我们回顾性地纳入了在意大利转诊中心连续住院的380例AHF患者,排除了严重三尖瓣反流的患者。受试者工作特征(ROC)曲线分析和Youden's J统计表明,sPAP≥48.75 mmHg是预测肺部(敏感性= 89.9%,特异性= 73%)和外周(敏感性= 88.3%,特异性= 82.5%)液体过载最准确的阈值。sPAP阈值与肺部和外周充血之间的关联经卡方检验证实(p p p = 0.012)。结论:sPAP阈值49 mmHg鉴别充血具有临床有用的准确性-肺(胸部x线)充血。
Systolic pulmonary artery pressure threshold to define pulmonary and peripheral congestion in acute heart failure in absence of severe tricuspid regurgitation.
Background and aims: Pulmonary and/or peripheral venous congestion defines the clinical diagnosis of acute heart failure (AHF). However, the systolic pulmonary arterial pressure (sPAP) thresholds at which pulmonary (chest x-ray) and inferior vena cava (IVC) congestion occur are not well established. This study aimed to identify a cut-off value of sPAP that reliably indicates AHF.
Methods and results: We retrospectively included 380 consecutive patients hospitalized for AHF at an Italian referral centre, after excluding those with severe tricuspid regurgitation. Receiver operating characteristic (ROC) curve analysis and Youden's J statistic identified a threshold of sPAP ≥ 48.75 mmHg as the most accurate in predicting both pulmonary (sensitivity = 89.9%, specificity = 73%) and peripheral (sensitivity = 88.3%, specificity = 82.5%) fluid overload. The association between this sPAP threshold and both pulmonary and peripheral congestion was confirmed by chi-square testing (p < 0.001) and multivariate logistic regression (p < 0.001). After adjustment for confounders, sPAP ≥ 49 mmHg was independently associated with all-cause death or heart failure (HF) hospitalization (HR = 1.713; 95% CI 1.127-2.602; p = 0.012).
Conclusions: sPAP threshold of 49 mmHg identifies congestion with clinically useful accuracy-pulmonary (chest X-ray) congestion.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


