{"title":"血浆纤维蛋白原水平与急性主动脉夹层预后——来自一项双中心队列研究的见解","authors":"Jiaxin Xiao, Junshuang Tang, Zilong Fu, Kaihong Yi, Xiulian Deng, Junsi Zheng, Qingqing Ni, Shiwan Wu, Yandan Xie, Weixing Huang, Yongquan Zhang, Xiao Wang, Liang Tao, Yequn Chen, Muli Wu","doi":"10.3389/fcvm.2025.1508749","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The relationship between plasma fibrinogen level (PFL) and prognosis of acute aortic dissection (AAD) are not well defined. The present study aimed to assess the effect of PFL on AAD prognosis through a two-center study and meta-analysis.</p><p><strong>Methods: </strong>A two-center cohort study was carried out in the two hospitals from Shantou and Xi'an cities. 1981 patients with AAD, admitted from 2012 to 2021, were included and followed up by clinical interview and telephone. The primary follow-up outcomes were 30-day mortality and long-term mortality. The relationship between PFL and all-cause mortality was identified. Further, meta-analysis was performed using our data and open access data.</p><p><strong>Results: </strong>The median follow-up time for the study cohort was 21.6 months (interquartile range 8.6-45.4 months). Compared with survivors, the non-survivors had a lower PFL. Survival analysis showed that mortality was higher in those with lower PFL. After multivariate adjustment, each 1 g/L increase in PFL was associated with a 18.9% decrease in 30-day mortality rate and a 11.5% decrease in long-term mortality rate (<i>P</i> < 0.001). Meta-analysis of the included our study revealed a significant association between lower PFL and increased 30-day mortality in type A and type B AAD [OR = 3.30, 95% CI: 2.58-4.23, <i>P</i> = 0.0739; <i>I</i> <sup>2</sup> = 47.9%]. Simultaneously, similar associations were observed in Stanford type A in for long-term mortality [OR = 3.62, 95% CI: 2.23-5.87, <i>P</i> = 0.0438; <i>I</i> <sup>2</sup> = 56.2%].</p><p><strong>Conclusions: </strong>Low PFL is a risk factor for short and long-term all-cause mortality in patients with type A AAD and short-term all-cause mortality in patients with type B AAD.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1508749"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500716/pdf/","citationCount":"0","resultStr":"{\"title\":\"Plasma fibrinogen level and acute aortic dissection prognosis-insights from a two-center cohort study.\",\"authors\":\"Jiaxin Xiao, Junshuang Tang, Zilong Fu, Kaihong Yi, Xiulian Deng, Junsi Zheng, Qingqing Ni, Shiwan Wu, Yandan Xie, Weixing Huang, Yongquan Zhang, Xiao Wang, Liang Tao, Yequn Chen, Muli Wu\",\"doi\":\"10.3389/fcvm.2025.1508749\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The relationship between plasma fibrinogen level (PFL) and prognosis of acute aortic dissection (AAD) are not well defined. The present study aimed to assess the effect of PFL on AAD prognosis through a two-center study and meta-analysis.</p><p><strong>Methods: </strong>A two-center cohort study was carried out in the two hospitals from Shantou and Xi'an cities. 1981 patients with AAD, admitted from 2012 to 2021, were included and followed up by clinical interview and telephone. The primary follow-up outcomes were 30-day mortality and long-term mortality. The relationship between PFL and all-cause mortality was identified. Further, meta-analysis was performed using our data and open access data.</p><p><strong>Results: </strong>The median follow-up time for the study cohort was 21.6 months (interquartile range 8.6-45.4 months). Compared with survivors, the non-survivors had a lower PFL. Survival analysis showed that mortality was higher in those with lower PFL. After multivariate adjustment, each 1 g/L increase in PFL was associated with a 18.9% decrease in 30-day mortality rate and a 11.5% decrease in long-term mortality rate (<i>P</i> < 0.001). Meta-analysis of the included our study revealed a significant association between lower PFL and increased 30-day mortality in type A and type B AAD [OR = 3.30, 95% CI: 2.58-4.23, <i>P</i> = 0.0739; <i>I</i> <sup>2</sup> = 47.9%]. Simultaneously, similar associations were observed in Stanford type A in for long-term mortality [OR = 3.62, 95% CI: 2.23-5.87, <i>P</i> = 0.0438; <i>I</i> <sup>2</sup> = 56.2%].</p><p><strong>Conclusions: </strong>Low PFL is a risk factor for short and long-term all-cause mortality in patients with type A AAD and short-term all-cause mortality in patients with type B AAD.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1508749\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500716/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1508749\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1508749","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Plasma fibrinogen level and acute aortic dissection prognosis-insights from a two-center cohort study.
Objective: The relationship between plasma fibrinogen level (PFL) and prognosis of acute aortic dissection (AAD) are not well defined. The present study aimed to assess the effect of PFL on AAD prognosis through a two-center study and meta-analysis.
Methods: A two-center cohort study was carried out in the two hospitals from Shantou and Xi'an cities. 1981 patients with AAD, admitted from 2012 to 2021, were included and followed up by clinical interview and telephone. The primary follow-up outcomes were 30-day mortality and long-term mortality. The relationship between PFL and all-cause mortality was identified. Further, meta-analysis was performed using our data and open access data.
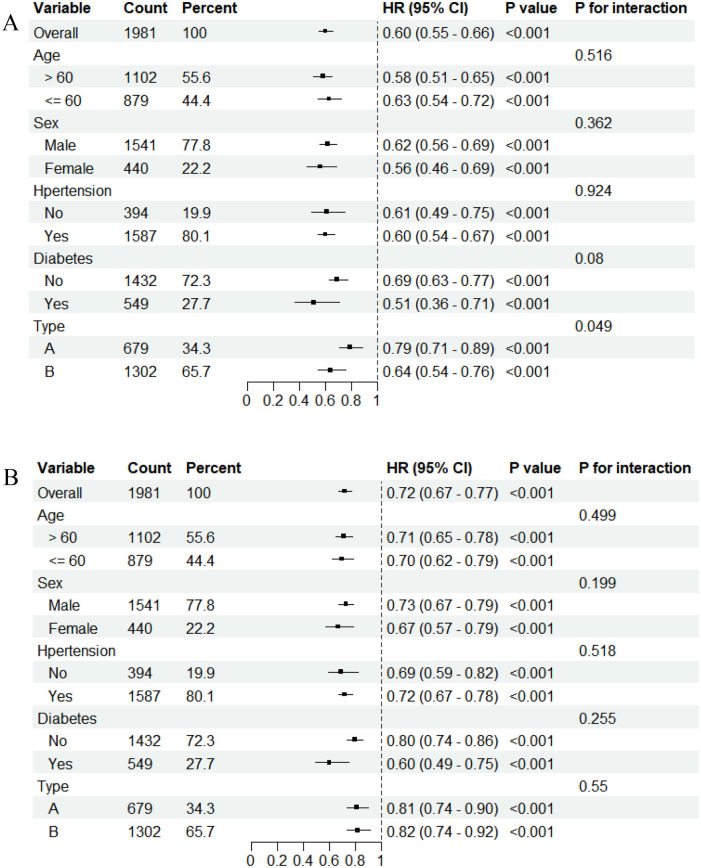
Results: The median follow-up time for the study cohort was 21.6 months (interquartile range 8.6-45.4 months). Compared with survivors, the non-survivors had a lower PFL. Survival analysis showed that mortality was higher in those with lower PFL. After multivariate adjustment, each 1 g/L increase in PFL was associated with a 18.9% decrease in 30-day mortality rate and a 11.5% decrease in long-term mortality rate (P < 0.001). Meta-analysis of the included our study revealed a significant association between lower PFL and increased 30-day mortality in type A and type B AAD [OR = 3.30, 95% CI: 2.58-4.23, P = 0.0739; I2 = 47.9%]. Simultaneously, similar associations were observed in Stanford type A in for long-term mortality [OR = 3.62, 95% CI: 2.23-5.87, P = 0.0438; I2 = 56.2%].
Conclusions: Low PFL is a risk factor for short and long-term all-cause mortality in patients with type A AAD and short-term all-cause mortality in patients with type B AAD.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


