{"title":"以重症肌无力为表现的咀嚼间隙原发性粘液表皮样癌。","authors":"Mitchell Boshkos, Sreya Rahman, Dharani Narendra","doi":"10.1159/000547406","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Myasthenia gravis (MG) is a neuromuscular autoimmune disorder, commonly associated with thymomas in the context of paraneoplastic syndromes. There are limited reports describing MG in the setting of non-thymic malignancies. Mucoepidermoid carcinoma (MEC), a malignancy of the salivary glands, has been underrecognized as a trigger for paraneoplastic MG. We present a case of a woman with new-onset MG and concurrent MEC of the left masticator space, representing a rare instance of paraneoplastic MG.</p><p><strong>Case presentation: </strong>A 24-year-old woman presented with a 9-month history of left-sided hemifacial twitching and facial and neck weakness, which progressed to drooling and dysphagia. Examination was notable for bilateral ptosis and fatigable weakness of bulbar and proximal limb muscles. During hospitalization, she developed worsening respiratory insufficiency, necessitating intubation for airway protection. Given concern for myasthenic crisis, empiric plasma exchange was initiated, with significant clinical improvement. Computerized tomography (CT) imaging of the neck revealed a mass within the left masticator space, and core needle biopsy established the diagnosis of MEC. Chest CT demonstrated no evidence of thymoma. Serologic evaluation revealed positive acetylcholine receptor binding and blocking antibodies, confirming a diagnosis of MG.</p><p><strong>Conclusion: </strong>The temporal relationship between MG symptoms and tumor discovery supports a paraneoplastic etiology in this patient. The occurrence of MG associated with non-thymic malignancies - particularly head and neck cancers - has only been reported twice. In MEC, the tumor may express antigens similar to those found in the neuromuscular junction in a process known as molecular mimicry. The immune system, in its attempt to target the tumor, inadvertently generates autoantibodies against these neuromuscular junction proteins, leading to the symptoms of MG. Whether resection of the tumor will lead to resolution of MG remains uncertain. Although no direct pathogenic link has been established between MEC and MG, this case suggests a need for increased clinical awareness and further investigation.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"1166-1170"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503555/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary Mucoepidermoid Carcinoma of the Masticator Space Presenting with Myasthenia Gravis.\",\"authors\":\"Mitchell Boshkos, Sreya Rahman, Dharani Narendra\",\"doi\":\"10.1159/000547406\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Myasthenia gravis (MG) is a neuromuscular autoimmune disorder, commonly associated with thymomas in the context of paraneoplastic syndromes. There are limited reports describing MG in the setting of non-thymic malignancies. Mucoepidermoid carcinoma (MEC), a malignancy of the salivary glands, has been underrecognized as a trigger for paraneoplastic MG. We present a case of a woman with new-onset MG and concurrent MEC of the left masticator space, representing a rare instance of paraneoplastic MG.</p><p><strong>Case presentation: </strong>A 24-year-old woman presented with a 9-month history of left-sided hemifacial twitching and facial and neck weakness, which progressed to drooling and dysphagia. Examination was notable for bilateral ptosis and fatigable weakness of bulbar and proximal limb muscles. During hospitalization, she developed worsening respiratory insufficiency, necessitating intubation for airway protection. Given concern for myasthenic crisis, empiric plasma exchange was initiated, with significant clinical improvement. Computerized tomography (CT) imaging of the neck revealed a mass within the left masticator space, and core needle biopsy established the diagnosis of MEC. Chest CT demonstrated no evidence of thymoma. Serologic evaluation revealed positive acetylcholine receptor binding and blocking antibodies, confirming a diagnosis of MG.</p><p><strong>Conclusion: </strong>The temporal relationship between MG symptoms and tumor discovery supports a paraneoplastic etiology in this patient. The occurrence of MG associated with non-thymic malignancies - particularly head and neck cancers - has only been reported twice. In MEC, the tumor may express antigens similar to those found in the neuromuscular junction in a process known as molecular mimicry. The immune system, in its attempt to target the tumor, inadvertently generates autoantibodies against these neuromuscular junction proteins, leading to the symptoms of MG. Whether resection of the tumor will lead to resolution of MG remains uncertain. Although no direct pathogenic link has been established between MEC and MG, this case suggests a need for increased clinical awareness and further investigation.</p>\",\"PeriodicalId\":9625,\"journal\":{\"name\":\"Case Reports in Oncology\",\"volume\":\"18 1\",\"pages\":\"1166-1170\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-07-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503555/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000547406\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000547406","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Primary Mucoepidermoid Carcinoma of the Masticator Space Presenting with Myasthenia Gravis.
Introduction: Myasthenia gravis (MG) is a neuromuscular autoimmune disorder, commonly associated with thymomas in the context of paraneoplastic syndromes. There are limited reports describing MG in the setting of non-thymic malignancies. Mucoepidermoid carcinoma (MEC), a malignancy of the salivary glands, has been underrecognized as a trigger for paraneoplastic MG. We present a case of a woman with new-onset MG and concurrent MEC of the left masticator space, representing a rare instance of paraneoplastic MG.
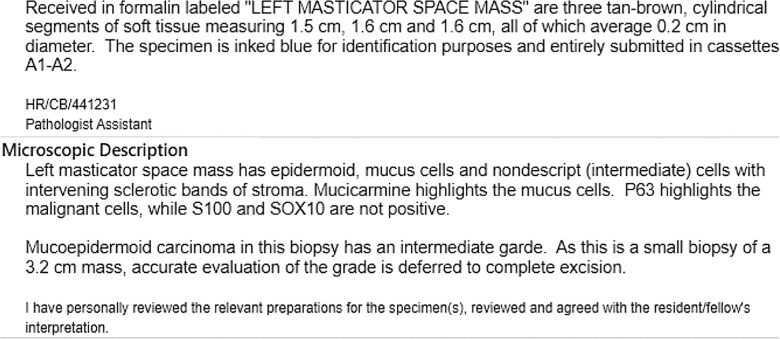
Case presentation: A 24-year-old woman presented with a 9-month history of left-sided hemifacial twitching and facial and neck weakness, which progressed to drooling and dysphagia. Examination was notable for bilateral ptosis and fatigable weakness of bulbar and proximal limb muscles. During hospitalization, she developed worsening respiratory insufficiency, necessitating intubation for airway protection. Given concern for myasthenic crisis, empiric plasma exchange was initiated, with significant clinical improvement. Computerized tomography (CT) imaging of the neck revealed a mass within the left masticator space, and core needle biopsy established the diagnosis of MEC. Chest CT demonstrated no evidence of thymoma. Serologic evaluation revealed positive acetylcholine receptor binding and blocking antibodies, confirming a diagnosis of MG.
Conclusion: The temporal relationship between MG symptoms and tumor discovery supports a paraneoplastic etiology in this patient. The occurrence of MG associated with non-thymic malignancies - particularly head and neck cancers - has only been reported twice. In MEC, the tumor may express antigens similar to those found in the neuromuscular junction in a process known as molecular mimicry. The immune system, in its attempt to target the tumor, inadvertently generates autoantibodies against these neuromuscular junction proteins, leading to the symptoms of MG. Whether resection of the tumor will lead to resolution of MG remains uncertain. Although no direct pathogenic link has been established between MEC and MG, this case suggests a need for increased clinical awareness and further investigation.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


