Xia Gong, Le Sang, Yunlei Huang, Hua Wang, Jian Sun
{"title":"脉冲振荡法检测慢性呼吸道症状患者小气道功能障碍、保留比受损肺活量测定法与COPD的关系","authors":"Xia Gong, Le Sang, Yunlei Huang, Hua Wang, Jian Sun","doi":"10.1186/s12890-025-03941-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Persistent chronic airway inflammation and progressive airflow limitation are typical features of chronic obstructive pulmonary disease (COPD). Emerging evidence indicates that small airway dysfunction (SAD) plays a critical role in driving the sustained pathological progression of COPD. Preserved ratio impaired spirometry (PRISm) represents a spirometric pattern characterized by a reduced forced expiratory volume in 1 second (FEV₁) despite a preserved ratio. Current evidence inadequately elucidates the pathophysiological role of SAD and its intricate interplay with PRISm and COPD progression. On the other hand, impulse oscillometry (IOS) can be used as a complementary tool to spirometry to detect SAD. Detection of SAD in patients with chronic respiratory symptoms could help in the diagnosis of PRISm and COPD when spirometry is not achievable.</p><p><strong>Objective: </strong>To investigate the diagnostic value of IOS for identifying SAD in patients with chronic respiratory symptoms, PRISm and COPD.</p><p><strong>Methods: </strong>Between September 2021 and July 2023, 552 symptomatic patients without known structural lung disease who underwent both spirometry and IOS on the same day in the outpatient clinic were evaluated. The correlations between spirometry and the IOS parameters, and the ROC curves of the IOS parameters for SAD patients and COPD patients were analyzed.</p><p><strong>Results: </strong>Among the 552 patients included in the study, 96 patients had COPD, 39 patients had PRISm, and 417 patients had chronic cough. Among 456 chronic cough patients with preserved ratio spirometry, the incidence of PRISm was 8.55%. Based on spirometry-defined SAD, the incidence of SAD in the PRISm population was 71.8%, which was significantly higher than the 9.35% of the non-PRISm population. With increasing COPD GOLD stage, the IOS parameters R5-R20, R5, Fres, and Ax increased, whereas the traditional lung function parameters and X5 decreased. R5-R20, X5, Fres, and AX of COPD GOLD stage 1 patients were not substantially different from those of PRISm patients. In PRISm patients, R5-R20, R5 and Fres were strongly correlated with FEF<sub>25%-75%</sub>. R5-R20, R5, X5, Fres and AX were significantly associated with FEV<sub>1</sub>, FEV<sub>1</sub>/FVC, FEV<sub>1</sub>% predicted, FEF<sub>50%</sub>, FEF<sub>75%</sub> and FEF<sub>25%-75%</sub> in COPD patients. Through ROC curve analysis, the cutoffs for identifying SAD in patients with chronic respiratory symptoms and PRISm patients were obtained, with R5-R20 values of 0.075 and 0.105 kPa/L/s, respectively. The values of R5 were 0.365 and 0.375 kPa/L/s, respectively. The Fres values are 16.31 Hz and 17.11 Hz, respectively. The cutoff for detecting COPD in all patients was 0.485 kPa/L/s for R5, 0.125 kPa/L/s for R5-R20, -0.155 kPa/L/s for X5, and 17.98 Hz for Fres. Fres had the highest AUC value for both SAD and COPD detection, and it detected COPD the most in all patients, with a prevalence of 24.1%. R5 detected SAD the most in patients with chronic respiratory symptoms, with a prevalence of 47.5%. With a prevalence of 71.8%, spirometry identified SAD in patients with PRISm the most frequently.</p><p><strong>Conclusion: </strong>Almost all IOS parameters Linked to the small airways were significantly different in the PRISm population compared with patients with chronic respiratory symptoms. SAD severity in PRISm patients is similar to that in GOLD stage 2 COPD patients. The IOS can assess the disease severity of COPD.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"458"},"PeriodicalIF":2.8000,"publicationDate":"2025-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12505595/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impulse oscillometry for the detection of small airway dysfunction in patients with chronic respiratory symptoms, preserved ratio impaired spirometry and COPD.\",\"authors\":\"Xia Gong, Le Sang, Yunlei Huang, Hua Wang, Jian Sun\",\"doi\":\"10.1186/s12890-025-03941-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Persistent chronic airway inflammation and progressive airflow limitation are typical features of chronic obstructive pulmonary disease (COPD). Emerging evidence indicates that small airway dysfunction (SAD) plays a critical role in driving the sustained pathological progression of COPD. Preserved ratio impaired spirometry (PRISm) represents a spirometric pattern characterized by a reduced forced expiratory volume in 1 second (FEV₁) despite a preserved ratio. Current evidence inadequately elucidates the pathophysiological role of SAD and its intricate interplay with PRISm and COPD progression. On the other hand, impulse oscillometry (IOS) can be used as a complementary tool to spirometry to detect SAD. Detection of SAD in patients with chronic respiratory symptoms could help in the diagnosis of PRISm and COPD when spirometry is not achievable.</p><p><strong>Objective: </strong>To investigate the diagnostic value of IOS for identifying SAD in patients with chronic respiratory symptoms, PRISm and COPD.</p><p><strong>Methods: </strong>Between September 2021 and July 2023, 552 symptomatic patients without known structural lung disease who underwent both spirometry and IOS on the same day in the outpatient clinic were evaluated. The correlations between spirometry and the IOS parameters, and the ROC curves of the IOS parameters for SAD patients and COPD patients were analyzed.</p><p><strong>Results: </strong>Among the 552 patients included in the study, 96 patients had COPD, 39 patients had PRISm, and 417 patients had chronic cough. Among 456 chronic cough patients with preserved ratio spirometry, the incidence of PRISm was 8.55%. Based on spirometry-defined SAD, the incidence of SAD in the PRISm population was 71.8%, which was significantly higher than the 9.35% of the non-PRISm population. With increasing COPD GOLD stage, the IOS parameters R5-R20, R5, Fres, and Ax increased, whereas the traditional lung function parameters and X5 decreased. R5-R20, X5, Fres, and AX of COPD GOLD stage 1 patients were not substantially different from those of PRISm patients. In PRISm patients, R5-R20, R5 and Fres were strongly correlated with FEF<sub>25%-75%</sub>. R5-R20, R5, X5, Fres and AX were significantly associated with FEV<sub>1</sub>, FEV<sub>1</sub>/FVC, FEV<sub>1</sub>% predicted, FEF<sub>50%</sub>, FEF<sub>75%</sub> and FEF<sub>25%-75%</sub> in COPD patients. Through ROC curve analysis, the cutoffs for identifying SAD in patients with chronic respiratory symptoms and PRISm patients were obtained, with R5-R20 values of 0.075 and 0.105 kPa/L/s, respectively. The values of R5 were 0.365 and 0.375 kPa/L/s, respectively. The Fres values are 16.31 Hz and 17.11 Hz, respectively. The cutoff for detecting COPD in all patients was 0.485 kPa/L/s for R5, 0.125 kPa/L/s for R5-R20, -0.155 kPa/L/s for X5, and 17.98 Hz for Fres. Fres had the highest AUC value for both SAD and COPD detection, and it detected COPD the most in all patients, with a prevalence of 24.1%. R5 detected SAD the most in patients with chronic respiratory symptoms, with a prevalence of 47.5%. With a prevalence of 71.8%, spirometry identified SAD in patients with PRISm the most frequently.</p><p><strong>Conclusion: </strong>Almost all IOS parameters Linked to the small airways were significantly different in the PRISm population compared with patients with chronic respiratory symptoms. SAD severity in PRISm patients is similar to that in GOLD stage 2 COPD patients. The IOS can assess the disease severity of COPD.</p>\",\"PeriodicalId\":9148,\"journal\":{\"name\":\"BMC Pulmonary Medicine\",\"volume\":\"25 1\",\"pages\":\"458\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-10-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12505595/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pulmonary Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12890-025-03941-1\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03941-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Impulse oscillometry for the detection of small airway dysfunction in patients with chronic respiratory symptoms, preserved ratio impaired spirometry and COPD.
Background: Persistent chronic airway inflammation and progressive airflow limitation are typical features of chronic obstructive pulmonary disease (COPD). Emerging evidence indicates that small airway dysfunction (SAD) plays a critical role in driving the sustained pathological progression of COPD. Preserved ratio impaired spirometry (PRISm) represents a spirometric pattern characterized by a reduced forced expiratory volume in 1 second (FEV₁) despite a preserved ratio. Current evidence inadequately elucidates the pathophysiological role of SAD and its intricate interplay with PRISm and COPD progression. On the other hand, impulse oscillometry (IOS) can be used as a complementary tool to spirometry to detect SAD. Detection of SAD in patients with chronic respiratory symptoms could help in the diagnosis of PRISm and COPD when spirometry is not achievable.
Objective: To investigate the diagnostic value of IOS for identifying SAD in patients with chronic respiratory symptoms, PRISm and COPD.
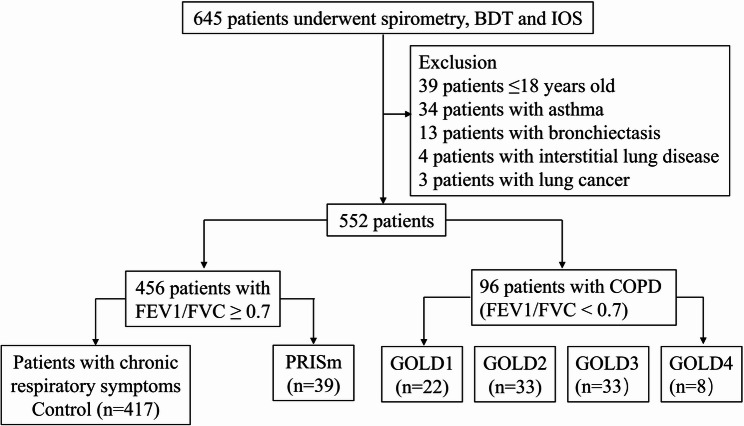
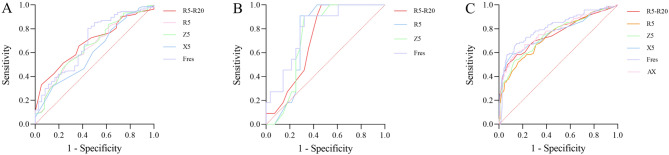
Methods: Between September 2021 and July 2023, 552 symptomatic patients without known structural lung disease who underwent both spirometry and IOS on the same day in the outpatient clinic were evaluated. The correlations between spirometry and the IOS parameters, and the ROC curves of the IOS parameters for SAD patients and COPD patients were analyzed.
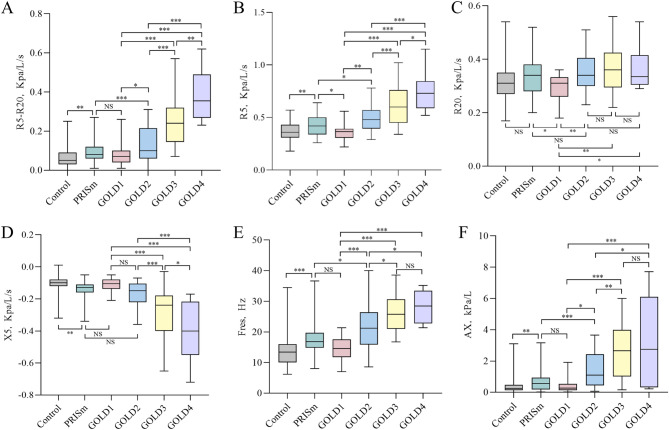
Results: Among the 552 patients included in the study, 96 patients had COPD, 39 patients had PRISm, and 417 patients had chronic cough. Among 456 chronic cough patients with preserved ratio spirometry, the incidence of PRISm was 8.55%. Based on spirometry-defined SAD, the incidence of SAD in the PRISm population was 71.8%, which was significantly higher than the 9.35% of the non-PRISm population. With increasing COPD GOLD stage, the IOS parameters R5-R20, R5, Fres, and Ax increased, whereas the traditional lung function parameters and X5 decreased. R5-R20, X5, Fres, and AX of COPD GOLD stage 1 patients were not substantially different from those of PRISm patients. In PRISm patients, R5-R20, R5 and Fres were strongly correlated with FEF25%-75%. R5-R20, R5, X5, Fres and AX were significantly associated with FEV1, FEV1/FVC, FEV1% predicted, FEF50%, FEF75% and FEF25%-75% in COPD patients. Through ROC curve analysis, the cutoffs for identifying SAD in patients with chronic respiratory symptoms and PRISm patients were obtained, with R5-R20 values of 0.075 and 0.105 kPa/L/s, respectively. The values of R5 were 0.365 and 0.375 kPa/L/s, respectively. The Fres values are 16.31 Hz and 17.11 Hz, respectively. The cutoff for detecting COPD in all patients was 0.485 kPa/L/s for R5, 0.125 kPa/L/s for R5-R20, -0.155 kPa/L/s for X5, and 17.98 Hz for Fres. Fres had the highest AUC value for both SAD and COPD detection, and it detected COPD the most in all patients, with a prevalence of 24.1%. R5 detected SAD the most in patients with chronic respiratory symptoms, with a prevalence of 47.5%. With a prevalence of 71.8%, spirometry identified SAD in patients with PRISm the most frequently.
Conclusion: Almost all IOS parameters Linked to the small airways were significantly different in the PRISm population compared with patients with chronic respiratory symptoms. SAD severity in PRISm patients is similar to that in GOLD stage 2 COPD patients. The IOS can assess the disease severity of COPD.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


