{"title":"钙化斑块患者的冠状动脉ct血管造影何时能准确?","authors":"Qisheng Ran, Diyou Chen, Huiru Zhang, Letian Zhang","doi":"10.3389/fcvm.2025.1570517","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To identify a new method to indicate when coronary computed tomography angiography (CCTA) in patients with calcified plaque can be accurate.</p><p><strong>Methods: </strong>Prospective analysis on 105 cases of coronary artery stenosis with calcified plaque underwent both CCTA and invasive coronary angiography (ICA). The Hounsfield unit (Hu) values of calcified plaque and adjacent blood were measured, and then the ratio (R <i><sub>Hu</sub></i> ) was subsequently calculated. The ICA data served as the gold standard for defining obstructive stenosis (≥ 50%) and were utilized to create a two-dimensional receiver operating characteristic (ROC) curve. The cut-off value was employed to categorize the CCTA data. Additionally, a Bland-Altman plot was used to analyze discrepancies in stenosis degree detection between CCTA and ICA. An <i>in vitro</i> experiment was designed to assess the practicability of R <i><sub>Hu</sub></i> .</p><p><strong>Results: </strong>The R <i><sub>Hu</sub></i> was correlated with the concordance of CCTA and ICA for stenosis evaluation (<i>r</i> = 0.509, <i>p</i> < 0.001). ROC analysis suggested a cut-off value of 0.36. The Bland-Altman plot indicated that stenosis evaluation by CCTA demonstrates good concordance when R <i><sub>Hu</sub></i> exceeds 0.36; however, significant bias occurs when R <i><sub>Hu</sub></i> is below 0.36 in comparison to ICA. <i>In vitro</i> experiments confirmed that the R <i><sub>Hu</sub></i> parameter can be easily adjusted to enhance the accuracy of CCTA. In validation experiments, the R <i><sub>Hu</sub></i> achieved a prediction accuracy of 74.0%.</p><p><strong>Conclusion: </strong>Our study suggests that the accuracy of detection of stenosis with CCTA in calcified vessels is related to the difference in Hu values between calcified plaques and blood.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1570517"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12497761/pdf/","citationCount":"0","resultStr":"{\"title\":\"When can coronary computed tomography angiography in patients with calcified plaque be accurate?\",\"authors\":\"Qisheng Ran, Diyou Chen, Huiru Zhang, Letian Zhang\",\"doi\":\"10.3389/fcvm.2025.1570517\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To identify a new method to indicate when coronary computed tomography angiography (CCTA) in patients with calcified plaque can be accurate.</p><p><strong>Methods: </strong>Prospective analysis on 105 cases of coronary artery stenosis with calcified plaque underwent both CCTA and invasive coronary angiography (ICA). The Hounsfield unit (Hu) values of calcified plaque and adjacent blood were measured, and then the ratio (R <i><sub>Hu</sub></i> ) was subsequently calculated. The ICA data served as the gold standard for defining obstructive stenosis (≥ 50%) and were utilized to create a two-dimensional receiver operating characteristic (ROC) curve. The cut-off value was employed to categorize the CCTA data. Additionally, a Bland-Altman plot was used to analyze discrepancies in stenosis degree detection between CCTA and ICA. An <i>in vitro</i> experiment was designed to assess the practicability of R <i><sub>Hu</sub></i> .</p><p><strong>Results: </strong>The R <i><sub>Hu</sub></i> was correlated with the concordance of CCTA and ICA for stenosis evaluation (<i>r</i> = 0.509, <i>p</i> < 0.001). ROC analysis suggested a cut-off value of 0.36. The Bland-Altman plot indicated that stenosis evaluation by CCTA demonstrates good concordance when R <i><sub>Hu</sub></i> exceeds 0.36; however, significant bias occurs when R <i><sub>Hu</sub></i> is below 0.36 in comparison to ICA. <i>In vitro</i> experiments confirmed that the R <i><sub>Hu</sub></i> parameter can be easily adjusted to enhance the accuracy of CCTA. In validation experiments, the R <i><sub>Hu</sub></i> achieved a prediction accuracy of 74.0%.</p><p><strong>Conclusion: </strong>Our study suggests that the accuracy of detection of stenosis with CCTA in calcified vessels is related to the difference in Hu values between calcified plaques and blood.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1570517\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12497761/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1570517\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1570517","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
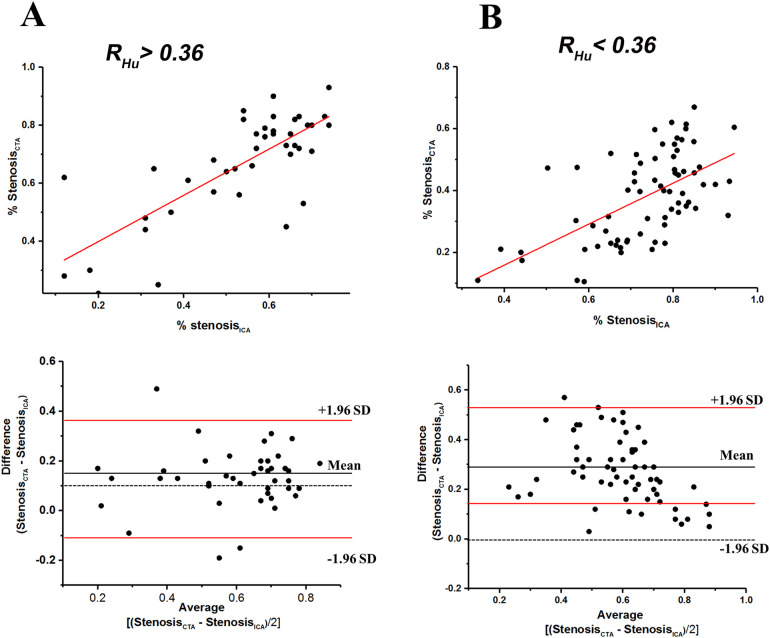
目的:寻找一种新的方法来确定钙化斑块患者的冠状动脉ct血管造影(CCTA)何时可以准确。方法:对105例冠状动脉狭窄合并钙化斑块行CCTA和有创冠状动脉造影(ICA)的患者进行前瞻性分析。测量钙化斑块与邻近血液的Hounsfield单位(Hu)值,计算其比值(R Hu)。ICA数据作为定义梗阻性狭窄(≥50%)的金标准,并用于创建二维受试者工作特征(ROC)曲线。采用截断值对CCTA数据进行分类。此外,使用Bland-Altman图分析CCTA和ICA之间狭窄程度检测的差异。设计体外实验,以评价其实用性。结果:R Hu与CCTA、ICA评价狭窄的一致性相关(R = 0.509, p Hu超过0.36),但R Hu小于0.36时与ICA比较存在显著偏倚。体外实验证实,R Hu参数可以很容易地进行调整,从而提高CCTA的准确性。在验证实验中,R Hu的预测准确率达到了74.0%。结论:本研究提示钙化血管CCTA检测狭窄的准确性与钙化斑块与血液的Hu值差异有关。
When can coronary computed tomography angiography in patients with calcified plaque be accurate?
Aim: To identify a new method to indicate when coronary computed tomography angiography (CCTA) in patients with calcified plaque can be accurate.
Methods: Prospective analysis on 105 cases of coronary artery stenosis with calcified plaque underwent both CCTA and invasive coronary angiography (ICA). The Hounsfield unit (Hu) values of calcified plaque and adjacent blood were measured, and then the ratio (R Hu ) was subsequently calculated. The ICA data served as the gold standard for defining obstructive stenosis (≥ 50%) and were utilized to create a two-dimensional receiver operating characteristic (ROC) curve. The cut-off value was employed to categorize the CCTA data. Additionally, a Bland-Altman plot was used to analyze discrepancies in stenosis degree detection between CCTA and ICA. An in vitro experiment was designed to assess the practicability of R Hu .
Results: The R Hu was correlated with the concordance of CCTA and ICA for stenosis evaluation (r = 0.509, p < 0.001). ROC analysis suggested a cut-off value of 0.36. The Bland-Altman plot indicated that stenosis evaluation by CCTA demonstrates good concordance when R Hu exceeds 0.36; however, significant bias occurs when R Hu is below 0.36 in comparison to ICA. In vitro experiments confirmed that the R Hu parameter can be easily adjusted to enhance the accuracy of CCTA. In validation experiments, the R Hu achieved a prediction accuracy of 74.0%.
Conclusion: Our study suggests that the accuracy of detection of stenosis with CCTA in calcified vessels is related to the difference in Hu values between calcified plaques and blood.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


