{"title":"大量不可修复的肩袖撕裂合并三角肌撕裂用反向全肩关节置换术治疗:病例报告和文献回顾。","authors":"Jianan Liu, Cheng Luo, Yanjuan Chen, Yijun He, Jiongfeng Huang","doi":"10.1097/MD.0000000000044507","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>Massive irreparable rotator cuff tear (IRCT) with concurrent deltoid tear poses a therapeutic challenge, as the deltoid compensates for lost rotator cuff function. Reverse total shoulder arthroplasty is often contraindicated, but emerging evidence supports its use with deltoid repair, even in patients with prior radiotherapy. This case addresses the knowledge gap in managing such complex cases.</p><p><strong>Patient concerns: </strong>A 67-year-old right-hand dominant male reported chronic right shoulder pain worsening after a fall, with limited range of motion (active flexion 40°, abduction 40°, extension 30°), a palpable middle deltoid gap, and supraspinatus/infraspinatus wasting. History included oral carcinoma resection, chemotherapy, and radiotherapy 3 years prior, without metastasis.</p><p><strong>Diagnoses: </strong>Massive IRCT of supraspinatus, infraspinatus, and subscapularis with retraction (Goutallier grade 3, Hamada 4b); 4-cm retracted middle deltoid tear; rotator cuff tear arthropathy with superior humeral head migration, acromial sclerosis, and glenohumeral degeneration, confirmed by x-ray, computed tomography, and magnetic resonance imaging. Preoperative Constant-Murley score: 27 (pain: 2, activities of daily living: 10, movement: 12, strength: 2).</p><p><strong>Interventions: </strong>One-stage reverse total shoulder arthroplasty with deltoid repair via deltopectoral incision extended along the anterolateral acromion. Deltoid stump reattached to acromion using transosseous sutures. Rehabilitation: 6 weeks immobilization at 90° abduction, followed by passive, active-assisted, and active range of motion exercises.</p><p><strong>Outcomes: </strong>At 1-year follow-up, pain resolved; active abduction/flexion improved to 165°, extension to 30°, with pain-free rotations. Postoperative Constant-Murley score: 93 (pain: 15, activities of daily living: 20, movement: 40, strength: 18). X-rays showed stable prosthesis without loosening or instability.</p><p><strong>Lessons: </strong>Reverse total shoulder arthroplasty with deltoid repair can achieve favorable short-term outcomes in IRCT with deltoid compromise, challenging traditional contraindications. Key factors include preserved anterior/posterior deltoid function, precise surgical techniques, and rehabilitation compliance. Long-term studies are needed for validation.</p>","PeriodicalId":18549,"journal":{"name":"Medicine","volume":"104 40","pages":"e44507"},"PeriodicalIF":1.4000,"publicationDate":"2025-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499805/pdf/","citationCount":"0","resultStr":"{\"title\":\"Massive irreparable rotator cuff tear with deltoid tear managed with reverse total shoulder arthroplasty: Case report and review of literature.\",\"authors\":\"Jianan Liu, Cheng Luo, Yanjuan Chen, Yijun He, Jiongfeng Huang\",\"doi\":\"10.1097/MD.0000000000044507\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Rationale: </strong>Massive irreparable rotator cuff tear (IRCT) with concurrent deltoid tear poses a therapeutic challenge, as the deltoid compensates for lost rotator cuff function. Reverse total shoulder arthroplasty is often contraindicated, but emerging evidence supports its use with deltoid repair, even in patients with prior radiotherapy. This case addresses the knowledge gap in managing such complex cases.</p><p><strong>Patient concerns: </strong>A 67-year-old right-hand dominant male reported chronic right shoulder pain worsening after a fall, with limited range of motion (active flexion 40°, abduction 40°, extension 30°), a palpable middle deltoid gap, and supraspinatus/infraspinatus wasting. History included oral carcinoma resection, chemotherapy, and radiotherapy 3 years prior, without metastasis.</p><p><strong>Diagnoses: </strong>Massive IRCT of supraspinatus, infraspinatus, and subscapularis with retraction (Goutallier grade 3, Hamada 4b); 4-cm retracted middle deltoid tear; rotator cuff tear arthropathy with superior humeral head migration, acromial sclerosis, and glenohumeral degeneration, confirmed by x-ray, computed tomography, and magnetic resonance imaging. Preoperative Constant-Murley score: 27 (pain: 2, activities of daily living: 10, movement: 12, strength: 2).</p><p><strong>Interventions: </strong>One-stage reverse total shoulder arthroplasty with deltoid repair via deltopectoral incision extended along the anterolateral acromion. Deltoid stump reattached to acromion using transosseous sutures. Rehabilitation: 6 weeks immobilization at 90° abduction, followed by passive, active-assisted, and active range of motion exercises.</p><p><strong>Outcomes: </strong>At 1-year follow-up, pain resolved; active abduction/flexion improved to 165°, extension to 30°, with pain-free rotations. Postoperative Constant-Murley score: 93 (pain: 15, activities of daily living: 20, movement: 40, strength: 18). X-rays showed stable prosthesis without loosening or instability.</p><p><strong>Lessons: </strong>Reverse total shoulder arthroplasty with deltoid repair can achieve favorable short-term outcomes in IRCT with deltoid compromise, challenging traditional contraindications. Key factors include preserved anterior/posterior deltoid function, precise surgical techniques, and rehabilitation compliance. Long-term studies are needed for validation.</p>\",\"PeriodicalId\":18549,\"journal\":{\"name\":\"Medicine\",\"volume\":\"104 40\",\"pages\":\"e44507\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499805/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/MD.0000000000044507\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/MD.0000000000044507","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Massive irreparable rotator cuff tear with deltoid tear managed with reverse total shoulder arthroplasty: Case report and review of literature.
Rationale: Massive irreparable rotator cuff tear (IRCT) with concurrent deltoid tear poses a therapeutic challenge, as the deltoid compensates for lost rotator cuff function. Reverse total shoulder arthroplasty is often contraindicated, but emerging evidence supports its use with deltoid repair, even in patients with prior radiotherapy. This case addresses the knowledge gap in managing such complex cases.
Patient concerns: A 67-year-old right-hand dominant male reported chronic right shoulder pain worsening after a fall, with limited range of motion (active flexion 40°, abduction 40°, extension 30°), a palpable middle deltoid gap, and supraspinatus/infraspinatus wasting. History included oral carcinoma resection, chemotherapy, and radiotherapy 3 years prior, without metastasis.
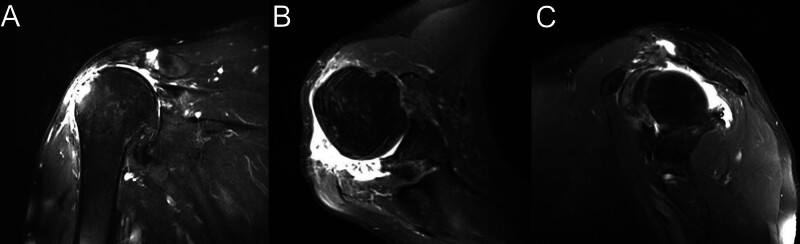
Diagnoses: Massive IRCT of supraspinatus, infraspinatus, and subscapularis with retraction (Goutallier grade 3, Hamada 4b); 4-cm retracted middle deltoid tear; rotator cuff tear arthropathy with superior humeral head migration, acromial sclerosis, and glenohumeral degeneration, confirmed by x-ray, computed tomography, and magnetic resonance imaging. Preoperative Constant-Murley score: 27 (pain: 2, activities of daily living: 10, movement: 12, strength: 2).
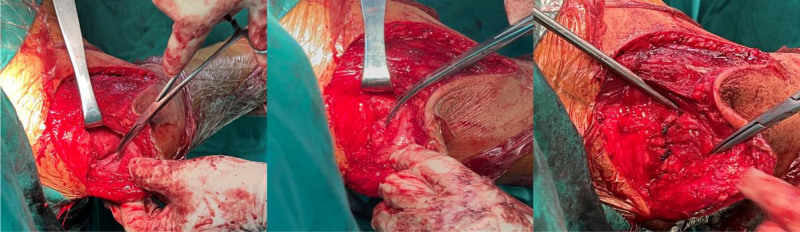
Interventions: One-stage reverse total shoulder arthroplasty with deltoid repair via deltopectoral incision extended along the anterolateral acromion. Deltoid stump reattached to acromion using transosseous sutures. Rehabilitation: 6 weeks immobilization at 90° abduction, followed by passive, active-assisted, and active range of motion exercises.
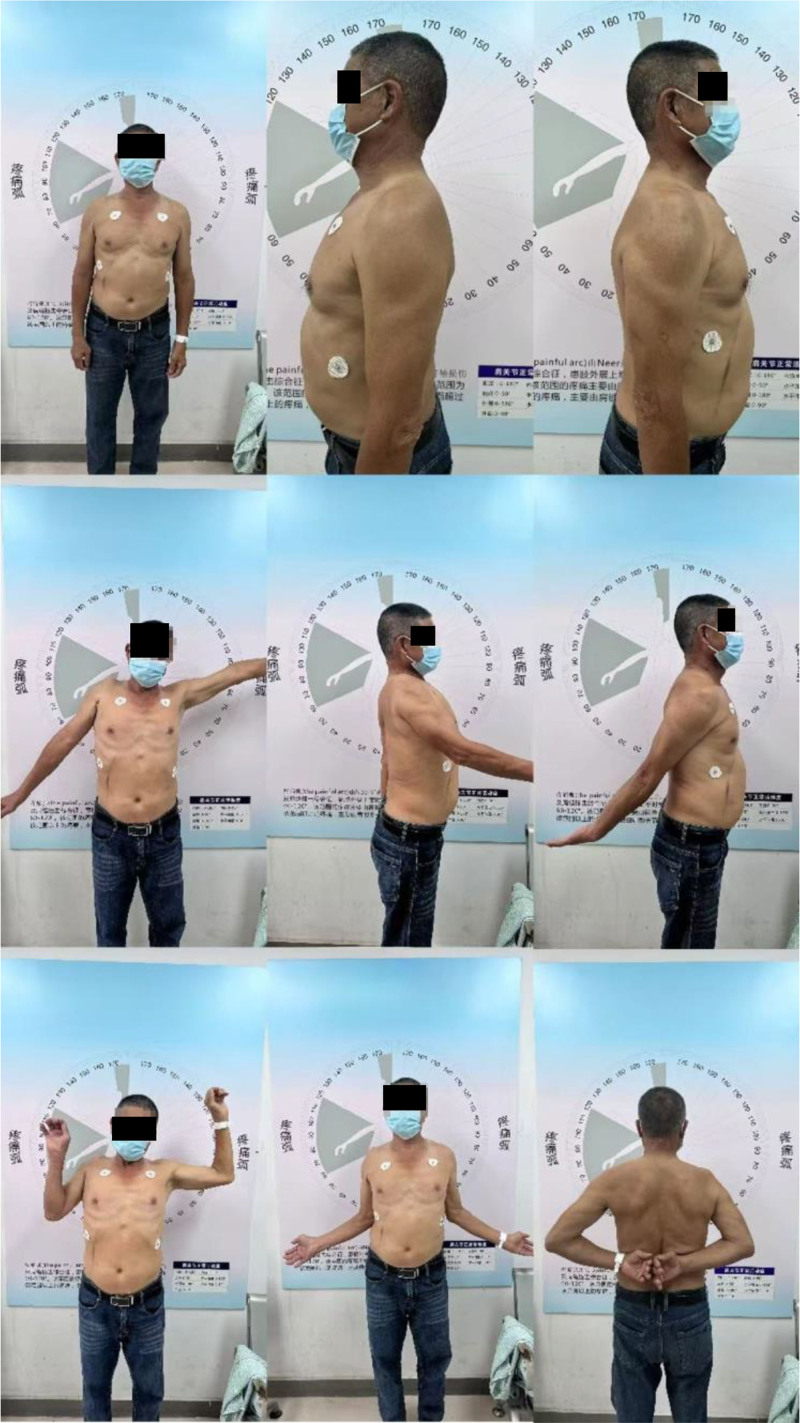
Outcomes: At 1-year follow-up, pain resolved; active abduction/flexion improved to 165°, extension to 30°, with pain-free rotations. Postoperative Constant-Murley score: 93 (pain: 15, activities of daily living: 20, movement: 40, strength: 18). X-rays showed stable prosthesis without loosening or instability.
Lessons: Reverse total shoulder arthroplasty with deltoid repair can achieve favorable short-term outcomes in IRCT with deltoid compromise, challenging traditional contraindications. Key factors include preserved anterior/posterior deltoid function, precise surgical techniques, and rehabilitation compliance. Long-term studies are needed for validation.
期刊介绍:
Medicine is now a fully open access journal, providing authors with a distinctive new service offering continuous publication of original research across a broad spectrum of medical scientific disciplines and sub-specialties.
As an open access title, Medicine will continue to provide authors with an established, trusted platform for the publication of their work. To ensure the ongoing quality of Medicine’s content, the peer-review process will only accept content that is scientifically, technically and ethically sound, and in compliance with standard reporting guidelines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


