Kathrine Kold Sørensen, Puriya Daniel Würtz Yazdanfard, Bochra Zareini, Ulrik Pedersen-Bjergaard, Vanja Kosjerina, Mikkel Porsborg Andersen, Anders Munch, Johan Sebastian Ohlendorff, Stefanie Schmid, Stefanie Lanzinger, Pratik Choudhary, Clare Gillies, Safoora Gharibzadeh, Marcus Lind, Viktor Tasselius, Jens Michelsen, Thomas Alexander Gerds, Christian Torp-Pedersen
{"title":"持续使用胰高血糖素样肽1 GLP-1受体激动剂治疗2型糖尿病的实际心血管效果","authors":"Kathrine Kold Sørensen, Puriya Daniel Würtz Yazdanfard, Bochra Zareini, Ulrik Pedersen-Bjergaard, Vanja Kosjerina, Mikkel Porsborg Andersen, Anders Munch, Johan Sebastian Ohlendorff, Stefanie Schmid, Stefanie Lanzinger, Pratik Choudhary, Clare Gillies, Safoora Gharibzadeh, Marcus Lind, Viktor Tasselius, Jens Michelsen, Thomas Alexander Gerds, Christian Torp-Pedersen","doi":"10.1186/s12933-025-02915-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular outcome trials have shown that glucagon-like peptide 1 receptor agonists (GLP1-RAs) reduce cardiovascular event rates more effectively than placebo and in patients with type 2 diabetes at increased cardiovascular risk. However, the generalizability of these findings to real-world settings remains uncertain.</p><p><strong>Aim: </strong>This study aimed to evaluate the real-world cardiovascular effectiveness of sustained GLP1-RA use compared to dipeptidyl peptidase 4 inhibitor (DPP-4i) over 3.5 years.</p><p><strong>Methods: </strong>Using Danish nationwide registries, we emulated a target trial to assess the real-world effectiveness of GLP1-RAs in a population of individuals with type 2 diabetes mirroring the inclusion and exclusion criteria from the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial. The study period was 2012-2022. Outcomes included the composite of myocardial infarction, stroke, and cardiovascular mortality (3P-MACE), as well as each component individually, alongside all-cause mortality, heart failure, angina pectoris, and revascularization. Longitudinal Targeted Minimum Loss-based Estimation, a method that adjusts for both baseline and time-varying confounding, was used to estimate absolute risks of cardiovascular outcomes under sustained use of GLP1-RA and DPP 4i (active comparator), adjusting for baseline and time-varying confounding.</p><p><strong>Results: </strong>We included 6,681 people initiating GLP1-RA and 19,072 initiating DPP-4i. Accounting for baseline and time-varying confounding, sustained GLP1-RA use showed a 2.5% (95% CI 0.8-4.1%) risk reduction of 3P-MACEover 3.5 years. Risk reductions for cardiovascular mortality, all-cause mortality, heart failure, and unstable angina pectoris were 2.3% (95% CI 1.4-3.1%), 2.5% (95% CI 0.7-4.3%), 0.9% (95% CI 0.01-1.8%), and 0.7% (95% CI 0.01-1.3%), respectively. No significant differences were observed for myocardial infarction, stroke, or revascularization with risk differences of 0.1% (95% CI -1.0 to 0.8%), 0.8% (95% CI -0.2 to 1.7%), and 0.2% (95% CI -0.7-1.1%), respectively.</p><p><strong>Conclusions: </strong>This real-world study confirms the cardiovascular benefits of GLP1-RAs over DPP-4is, particularly for reducing cardiovascular and all-cause mortality under continuous treatment exposure in patients with type 2 diabetes at increased cardiovascular risk.</p>","PeriodicalId":9374,"journal":{"name":"Cardiovascular Diabetology","volume":"24 1","pages":"385"},"PeriodicalIF":10.6000,"publicationDate":"2025-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502128/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world cardiovascular effectiveness of sustained glucagon-like peptide 1 GLP-1 receptor agonist usage in type 2 diabetes.\",\"authors\":\"Kathrine Kold Sørensen, Puriya Daniel Würtz Yazdanfard, Bochra Zareini, Ulrik Pedersen-Bjergaard, Vanja Kosjerina, Mikkel Porsborg Andersen, Anders Munch, Johan Sebastian Ohlendorff, Stefanie Schmid, Stefanie Lanzinger, Pratik Choudhary, Clare Gillies, Safoora Gharibzadeh, Marcus Lind, Viktor Tasselius, Jens Michelsen, Thomas Alexander Gerds, Christian Torp-Pedersen\",\"doi\":\"10.1186/s12933-025-02915-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiovascular outcome trials have shown that glucagon-like peptide 1 receptor agonists (GLP1-RAs) reduce cardiovascular event rates more effectively than placebo and in patients with type 2 diabetes at increased cardiovascular risk. However, the generalizability of these findings to real-world settings remains uncertain.</p><p><strong>Aim: </strong>This study aimed to evaluate the real-world cardiovascular effectiveness of sustained GLP1-RA use compared to dipeptidyl peptidase 4 inhibitor (DPP-4i) over 3.5 years.</p><p><strong>Methods: </strong>Using Danish nationwide registries, we emulated a target trial to assess the real-world effectiveness of GLP1-RAs in a population of individuals with type 2 diabetes mirroring the inclusion and exclusion criteria from the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial. The study period was 2012-2022. Outcomes included the composite of myocardial infarction, stroke, and cardiovascular mortality (3P-MACE), as well as each component individually, alongside all-cause mortality, heart failure, angina pectoris, and revascularization. Longitudinal Targeted Minimum Loss-based Estimation, a method that adjusts for both baseline and time-varying confounding, was used to estimate absolute risks of cardiovascular outcomes under sustained use of GLP1-RA and DPP 4i (active comparator), adjusting for baseline and time-varying confounding.</p><p><strong>Results: </strong>We included 6,681 people initiating GLP1-RA and 19,072 initiating DPP-4i. Accounting for baseline and time-varying confounding, sustained GLP1-RA use showed a 2.5% (95% CI 0.8-4.1%) risk reduction of 3P-MACEover 3.5 years. Risk reductions for cardiovascular mortality, all-cause mortality, heart failure, and unstable angina pectoris were 2.3% (95% CI 1.4-3.1%), 2.5% (95% CI 0.7-4.3%), 0.9% (95% CI 0.01-1.8%), and 0.7% (95% CI 0.01-1.3%), respectively. No significant differences were observed for myocardial infarction, stroke, or revascularization with risk differences of 0.1% (95% CI -1.0 to 0.8%), 0.8% (95% CI -0.2 to 1.7%), and 0.2% (95% CI -0.7-1.1%), respectively.</p><p><strong>Conclusions: </strong>This real-world study confirms the cardiovascular benefits of GLP1-RAs over DPP-4is, particularly for reducing cardiovascular and all-cause mortality under continuous treatment exposure in patients with type 2 diabetes at increased cardiovascular risk.</p>\",\"PeriodicalId\":9374,\"journal\":{\"name\":\"Cardiovascular Diabetology\",\"volume\":\"24 1\",\"pages\":\"385\"},\"PeriodicalIF\":10.6000,\"publicationDate\":\"2025-10-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502128/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular Diabetology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12933-025-02915-1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Diabetology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12933-025-02915-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:心血管结局试验表明,胰高血糖素样肽1受体激动剂(GLP1-RAs)在心血管风险增加的2型糖尿病患者中比安慰剂更有效地降低心血管事件发生率。然而,这些发现在现实世界中的普遍性仍然不确定。目的:本研究旨在评估持续使用GLP1-RA与二肽基肽酶4抑制剂(DPP-4i)超过3.5年的实际心血管疗效。方法:使用丹麦全国注册中心,我们模拟了一项目标试验,以评估GLP1-RAs在2型糖尿病患者群体中的实际有效性,这反映了利拉鲁肽在糖尿病中的作用和作用:心血管结局结果评估(LEADER)试验的纳入和排除标准。研究期间为2012-2022年。结果包括心肌梗死、卒中和心血管死亡率(3P-MACE)的组合,以及每个组成部分单独,以及全因死亡率、心力衰竭、心绞痛和血运重建。纵向目标最小损失估计是一种调整基线和时变混杂因素的方法,用于估计持续使用GLP1-RA和DPP 4i(活性比较剂)时心血管结果的绝对风险,调整基线和时变混杂因素。结果:我们纳入了6681例GLP1-RA患者和19072例DPP-4i患者。考虑到基线和时变的混杂因素,持续使用GLP1-RA显示3.5年以上3p - mace2.5 % (95% CI 0.8-4.1%)的风险降低。心血管死亡率、全因死亡率、心力衰竭和不稳定型心绞痛的风险降低分别为2.3% (95% CI 1.4-3.1%)、2.5% (95% CI 0.7-4.3%)、0.9% (95% CI 0.01-1.8%)和0.7% (95% CI 0.01-1.3%)。心肌梗死、卒中或血运重建术的风险差异分别为0.1% (95% CI -1.0 ~ 0.8%)、0.8% (95% CI -0.2 ~ 1.7%)和0.2% (95% CI -0.7 ~ 1.1%),无显著差异。结论:这项现实世界的研究证实了GLP1-RAs比DPP-4is对心血管的益处,特别是在心血管风险增加的2型糖尿病患者持续接受治疗时降低心血管和全因死亡率。
Real-world cardiovascular effectiveness of sustained glucagon-like peptide 1 GLP-1 receptor agonist usage in type 2 diabetes.
Background: Cardiovascular outcome trials have shown that glucagon-like peptide 1 receptor agonists (GLP1-RAs) reduce cardiovascular event rates more effectively than placebo and in patients with type 2 diabetes at increased cardiovascular risk. However, the generalizability of these findings to real-world settings remains uncertain.
Aim: This study aimed to evaluate the real-world cardiovascular effectiveness of sustained GLP1-RA use compared to dipeptidyl peptidase 4 inhibitor (DPP-4i) over 3.5 years.
Methods: Using Danish nationwide registries, we emulated a target trial to assess the real-world effectiveness of GLP1-RAs in a population of individuals with type 2 diabetes mirroring the inclusion and exclusion criteria from the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial. The study period was 2012-2022. Outcomes included the composite of myocardial infarction, stroke, and cardiovascular mortality (3P-MACE), as well as each component individually, alongside all-cause mortality, heart failure, angina pectoris, and revascularization. Longitudinal Targeted Minimum Loss-based Estimation, a method that adjusts for both baseline and time-varying confounding, was used to estimate absolute risks of cardiovascular outcomes under sustained use of GLP1-RA and DPP 4i (active comparator), adjusting for baseline and time-varying confounding.
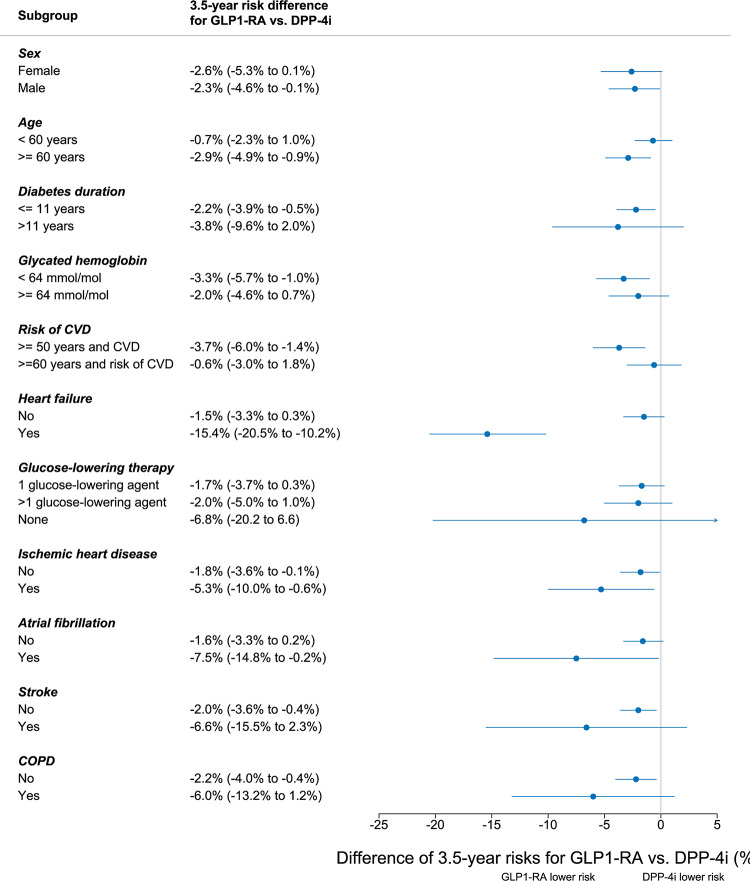
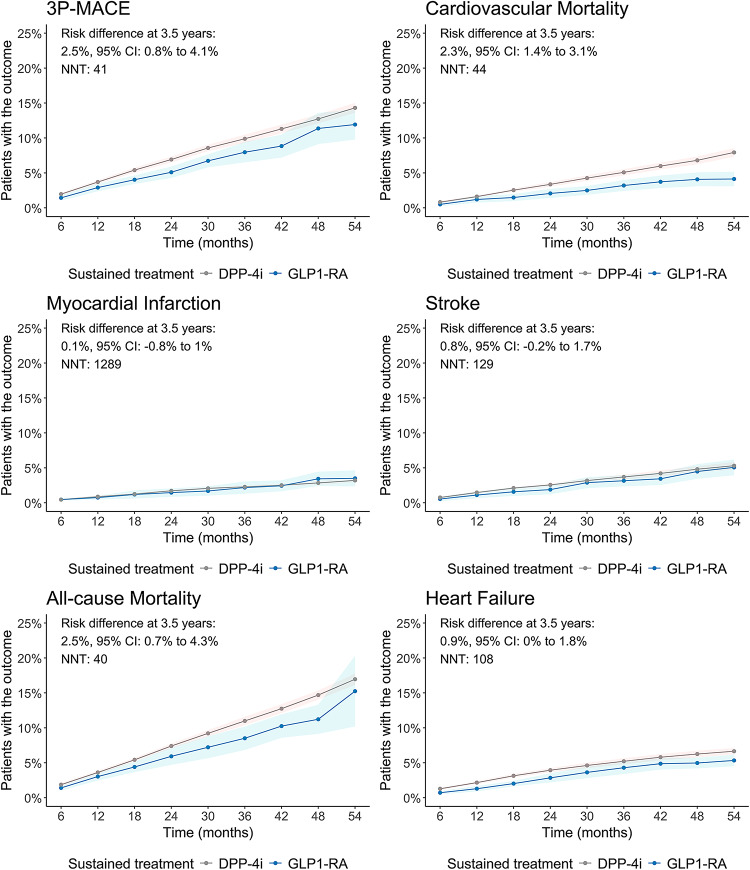
Results: We included 6,681 people initiating GLP1-RA and 19,072 initiating DPP-4i. Accounting for baseline and time-varying confounding, sustained GLP1-RA use showed a 2.5% (95% CI 0.8-4.1%) risk reduction of 3P-MACEover 3.5 years. Risk reductions for cardiovascular mortality, all-cause mortality, heart failure, and unstable angina pectoris were 2.3% (95% CI 1.4-3.1%), 2.5% (95% CI 0.7-4.3%), 0.9% (95% CI 0.01-1.8%), and 0.7% (95% CI 0.01-1.3%), respectively. No significant differences were observed for myocardial infarction, stroke, or revascularization with risk differences of 0.1% (95% CI -1.0 to 0.8%), 0.8% (95% CI -0.2 to 1.7%), and 0.2% (95% CI -0.7-1.1%), respectively.
Conclusions: This real-world study confirms the cardiovascular benefits of GLP1-RAs over DPP-4is, particularly for reducing cardiovascular and all-cause mortality under continuous treatment exposure in patients with type 2 diabetes at increased cardiovascular risk.
期刊介绍:
Cardiovascular Diabetology is a journal that welcomes manuscripts exploring various aspects of the relationship between diabetes, cardiovascular health, and the metabolic syndrome. We invite submissions related to clinical studies, genetic investigations, experimental research, pharmacological studies, epidemiological analyses, and molecular biology research in this field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


