{"title":"外科重症监护病房接受机械通气患者的机械功率及其与死亡率增加的关系:一项回顾性队列研究","authors":"Annop Piriyapatsom, Ajana Trisukhonth, Ornin Chintabanyat, Chayanan Thanakiattiwibun","doi":"10.1136/bmjresp-2024-002843","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A potential correlation between mechanical power (MP) and clinical outcomes in mechanically ventilated patients has been reported. Limited data exist regarding MP among patients admitted to surgical intensive care units (SICUs) who require mechanical ventilation (MV) support. The primary objective of this study was to determine MP in mechanically ventilated patients admitted to the SICU, and the secondary objective was to explore whether MP was associated with clinical outcomes.</p><p><strong>Methods: </strong>This retrospective cohort study conducted at the SICU of the tertiary university-based hospital included 283 postoperative patients admitted to the SICU who required MV support for ≥12 hours. Ventilator parameters were recorded at MV initiation and 24 hours, and MP was subsequently computed. Cox regression analysis was employed to assess the association between MP and 90-day mortality.</p><p><strong>Results: </strong>MP at MV initiation and 24 hours were median 11.9 (IQR 8.6-17.1) J/min and 11.9 (8.9-16.8) J/min, respectively. MP was significantly higher in non-survivors both at MV initiation and 24 hours (15.4 (12.5-21.2) J/min vs 11 (8.3-15.6) J/min, p<0.001 and 15.9 (10.6-20.2) J/min vs 10.9 (8.5-15.4) J/min, p=0.001, respectively). MP ≥12 J/min at MV initiation was associated with increased 90-day mortality (HR 2.21, 95% CI 1.09 to 4.48), particularly among patients with high acuity, those at a high risk of acute lung injury and those who did not receive lung protective ventilation. In patients with MP ≥12 J/min at MV initiation, a subsequent rise in MP of ≥5 J/min at 24 hours was correlated with accentuated 90-day mortality.</p><p><strong>Conclusion: </strong>Among mechanically ventilated patients in the SICU, MP at the initiation and at 24 hours of MV support was approximately 12 J/min. An elevated MP was an independent predictor of elevated 90-day mortality, especially in cases with high illness acuity. Alterations in MP during MV support could impact the 90-day mortality in these individuals.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506055/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mechanical power in patients receiving mechanical ventilation in the surgical intensive care unit and its association with increased mortality: a retrospective cohort study.\",\"authors\":\"Annop Piriyapatsom, Ajana Trisukhonth, Ornin Chintabanyat, Chayanan Thanakiattiwibun\",\"doi\":\"10.1136/bmjresp-2024-002843\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>A potential correlation between mechanical power (MP) and clinical outcomes in mechanically ventilated patients has been reported. Limited data exist regarding MP among patients admitted to surgical intensive care units (SICUs) who require mechanical ventilation (MV) support. The primary objective of this study was to determine MP in mechanically ventilated patients admitted to the SICU, and the secondary objective was to explore whether MP was associated with clinical outcomes.</p><p><strong>Methods: </strong>This retrospective cohort study conducted at the SICU of the tertiary university-based hospital included 283 postoperative patients admitted to the SICU who required MV support for ≥12 hours. Ventilator parameters were recorded at MV initiation and 24 hours, and MP was subsequently computed. Cox regression analysis was employed to assess the association between MP and 90-day mortality.</p><p><strong>Results: </strong>MP at MV initiation and 24 hours were median 11.9 (IQR 8.6-17.1) J/min and 11.9 (8.9-16.8) J/min, respectively. MP was significantly higher in non-survivors both at MV initiation and 24 hours (15.4 (12.5-21.2) J/min vs 11 (8.3-15.6) J/min, p<0.001 and 15.9 (10.6-20.2) J/min vs 10.9 (8.5-15.4) J/min, p=0.001, respectively). MP ≥12 J/min at MV initiation was associated with increased 90-day mortality (HR 2.21, 95% CI 1.09 to 4.48), particularly among patients with high acuity, those at a high risk of acute lung injury and those who did not receive lung protective ventilation. In patients with MP ≥12 J/min at MV initiation, a subsequent rise in MP of ≥5 J/min at 24 hours was correlated with accentuated 90-day mortality.</p><p><strong>Conclusion: </strong>Among mechanically ventilated patients in the SICU, MP at the initiation and at 24 hours of MV support was approximately 12 J/min. An elevated MP was an independent predictor of elevated 90-day mortality, especially in cases with high illness acuity. Alterations in MP during MV support could impact the 90-day mortality in these individuals.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506055/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2024-002843\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002843","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
导读:机械通气患者的机械功率(MP)与临床结果之间存在潜在的相关性。关于外科重症监护病房(sicu)中需要机械通气(MV)支持的患者的MP数据有限。本研究的主要目的是确定SICU机械通气患者的MP,次要目的是探讨MP是否与临床结果相关。方法:本回顾性队列研究在第三大学附属医院SICU进行,纳入283例需要MV支持≥12小时的SICU术后患者。记录呼吸机在MV起始和24小时的参数,随后计算MP。采用Cox回归分析评估MP与90天死亡率之间的关系。结果:MV起始和24小时时MP的中位值分别为11.9 (IQR 8.6-17.1) J/min和11.9 (8.9-16.8)J/min。结论:在SICU的机械通气患者中,开始和24小时时的MP均显著高于非幸存者(15.4 (12.5-21.2)J/min vs 11 (8.3-15.6) J/min)。MP升高是90天死亡率升高的独立预测因子,特别是在疾病急性度高的病例中。在MV支持期间MP的改变可能影响这些个体的90天死亡率。
Mechanical power in patients receiving mechanical ventilation in the surgical intensive care unit and its association with increased mortality: a retrospective cohort study.
Introduction: A potential correlation between mechanical power (MP) and clinical outcomes in mechanically ventilated patients has been reported. Limited data exist regarding MP among patients admitted to surgical intensive care units (SICUs) who require mechanical ventilation (MV) support. The primary objective of this study was to determine MP in mechanically ventilated patients admitted to the SICU, and the secondary objective was to explore whether MP was associated with clinical outcomes.
Methods: This retrospective cohort study conducted at the SICU of the tertiary university-based hospital included 283 postoperative patients admitted to the SICU who required MV support for ≥12 hours. Ventilator parameters were recorded at MV initiation and 24 hours, and MP was subsequently computed. Cox regression analysis was employed to assess the association between MP and 90-day mortality.
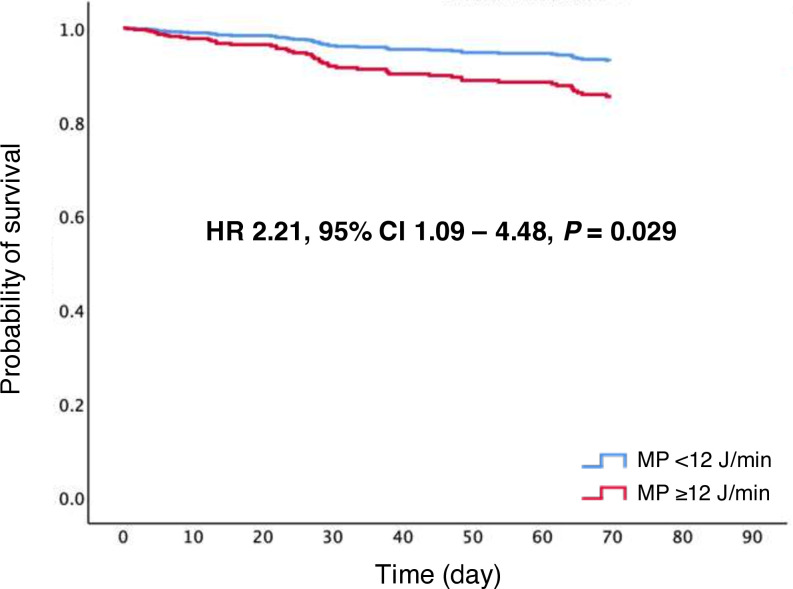
Results: MP at MV initiation and 24 hours were median 11.9 (IQR 8.6-17.1) J/min and 11.9 (8.9-16.8) J/min, respectively. MP was significantly higher in non-survivors both at MV initiation and 24 hours (15.4 (12.5-21.2) J/min vs 11 (8.3-15.6) J/min, p<0.001 and 15.9 (10.6-20.2) J/min vs 10.9 (8.5-15.4) J/min, p=0.001, respectively). MP ≥12 J/min at MV initiation was associated with increased 90-day mortality (HR 2.21, 95% CI 1.09 to 4.48), particularly among patients with high acuity, those at a high risk of acute lung injury and those who did not receive lung protective ventilation. In patients with MP ≥12 J/min at MV initiation, a subsequent rise in MP of ≥5 J/min at 24 hours was correlated with accentuated 90-day mortality.
Conclusion: Among mechanically ventilated patients in the SICU, MP at the initiation and at 24 hours of MV support was approximately 12 J/min. An elevated MP was an independent predictor of elevated 90-day mortality, especially in cases with high illness acuity. Alterations in MP during MV support could impact the 90-day mortality in these individuals.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


