{"title":"系统性免疫炎症指数与股骨头骨坏死核心减压后失败的关联:一项前瞻性事件时间分析","authors":"Chengsi Li, Haichuan Guo, Ziyu Han, Tianyu Wang, Dongwei Wu, Zhenbang Yang, Xinqun Cheng, Yingze Zhang, Yanbin Zhu","doi":"10.1080/07853890.2025.2566867","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to assess the association between preoperative systemic immune inflammation index (SII) and failure after core decompression (CD).</p><p><strong>Methods: </strong>We conducted a prospective study of patients admitted to a tertiary referral hospital with osteonecrosis of the femoral head who underwent CD between October 1, 2014 and April 30, 2019, and provided a minimum 3-year follow-up assessment. Restricted cubic splines assessed the dose-effect relationship between SII and failure. Propensity score matching (PSM) balanced potential preoperative confounders. Kaplan-Meier analyses estimated cumulative incidence as a function of time for the failure between low SII and high SII groups. Multivariable Cox proportional hazards models evaluated the independent association of high SII with failure after adjustment for perioperative factors. Prespecified subgroup analyses explored heterogeneity.</p><p><strong>Results: </strong>We found a positive relationship between the preoperative SII and failure after CD. Among 963 CD procedures performed in 676 patients, failure was observed in 97 cases in a median period of 5.4 years. The cumulative incidence of failure was 10.6% (95% CI, 8.7%, 12.8%) at 5 years. After PSM, failure rates at 5 years were identified as significant differences between the high SII and low SII groups (Log-rank p = 0.019), and that high SII was independently associated with a 1.90-fold (95% CI, 1.14, 3.18; p = 0.014) increased risk of failure. Significant heterogeneity was observed by gender and aetiology (P for interaction < 0.05).</p><p><strong>Conclusions: </strong>Preoperative high SII is a significant risk factor for failure after CD, which could be considered when evaluating surgical indications and providing preoperative counseling to patients.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2566867"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502117/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of the systemic immune inflammation index with failure after core decompression for osteonecrosis of the femoral head: a prospective time-to-event analysis.\",\"authors\":\"Chengsi Li, Haichuan Guo, Ziyu Han, Tianyu Wang, Dongwei Wu, Zhenbang Yang, Xinqun Cheng, Yingze Zhang, Yanbin Zhu\",\"doi\":\"10.1080/07853890.2025.2566867\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aimed to assess the association between preoperative systemic immune inflammation index (SII) and failure after core decompression (CD).</p><p><strong>Methods: </strong>We conducted a prospective study of patients admitted to a tertiary referral hospital with osteonecrosis of the femoral head who underwent CD between October 1, 2014 and April 30, 2019, and provided a minimum 3-year follow-up assessment. Restricted cubic splines assessed the dose-effect relationship between SII and failure. Propensity score matching (PSM) balanced potential preoperative confounders. Kaplan-Meier analyses estimated cumulative incidence as a function of time for the failure between low SII and high SII groups. Multivariable Cox proportional hazards models evaluated the independent association of high SII with failure after adjustment for perioperative factors. Prespecified subgroup analyses explored heterogeneity.</p><p><strong>Results: </strong>We found a positive relationship between the preoperative SII and failure after CD. Among 963 CD procedures performed in 676 patients, failure was observed in 97 cases in a median period of 5.4 years. The cumulative incidence of failure was 10.6% (95% CI, 8.7%, 12.8%) at 5 years. After PSM, failure rates at 5 years were identified as significant differences between the high SII and low SII groups (Log-rank p = 0.019), and that high SII was independently associated with a 1.90-fold (95% CI, 1.14, 3.18; p = 0.014) increased risk of failure. Significant heterogeneity was observed by gender and aetiology (P for interaction < 0.05).</p><p><strong>Conclusions: </strong>Preoperative high SII is a significant risk factor for failure after CD, which could be considered when evaluating surgical indications and providing preoperative counseling to patients.</p>\",\"PeriodicalId\":93874,\"journal\":{\"name\":\"Annals of medicine\",\"volume\":\"57 1\",\"pages\":\"2566867\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502117/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/07853890.2025.2566867\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2566867","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究旨在评估术前全身免疫炎症指数(SII)与核心减压(CD)后衰竭的关系。方法:我们对2014年10月1日至2019年4月30日期间在三级转诊医院接受CD治疗的股骨头坏死患者进行了一项前瞻性研究,并提供了至少3年的随访评估。受限三次样条评估了SII和失效之间的剂量效应关系。倾向评分匹配(PSM)平衡了潜在的术前混杂因素。Kaplan-Meier分析估计了低SII组和高SII组之间的累积发生率作为失败时间的函数。多变量Cox比例风险模型评估围手术期因素调整后高SII与失败的独立关联。预先指定的亚组分析探讨异质性。结果:我们发现术前SII与CD后失败呈正相关。在676例患者进行的963例CD手术中,有97例患者在中位5.4年的时间内观察到失败。5年累计失败率为10.6% (95% CI, 8.7%, 12.8%)。PSM后,5年的失败率在高SII组和低SII组之间被确定为显著差异(Log-rank p = 0.019),高SII与1.90倍(95% CI, 1.14, 3.18; p = 0.014)的失败风险增加独立相关。性别和病因差异有统计学意义(交互作用P < 0.05)。结论:术前高SII是CD术后失败的重要危险因素,在评估手术指征和提供术前咨询时应予以考虑。
Association of the systemic immune inflammation index with failure after core decompression for osteonecrosis of the femoral head: a prospective time-to-event analysis.
Objective: This study aimed to assess the association between preoperative systemic immune inflammation index (SII) and failure after core decompression (CD).
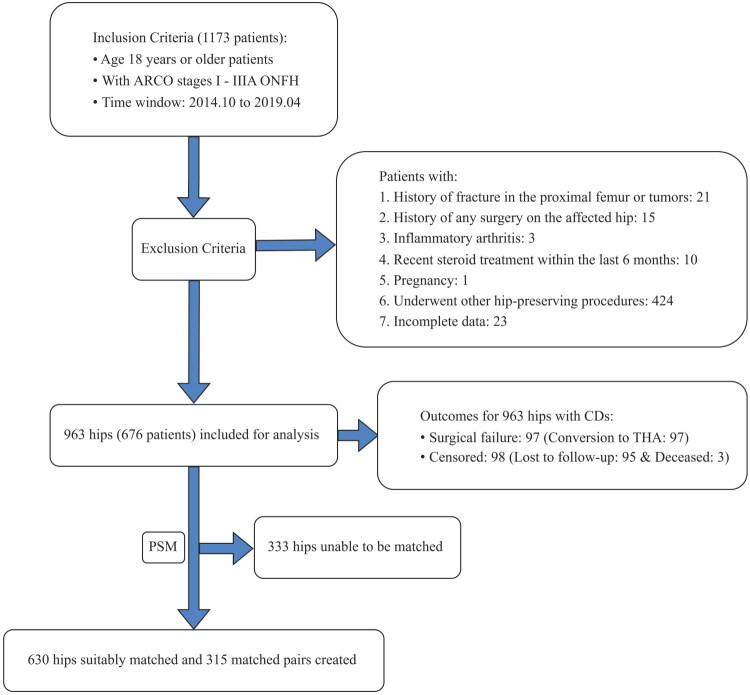
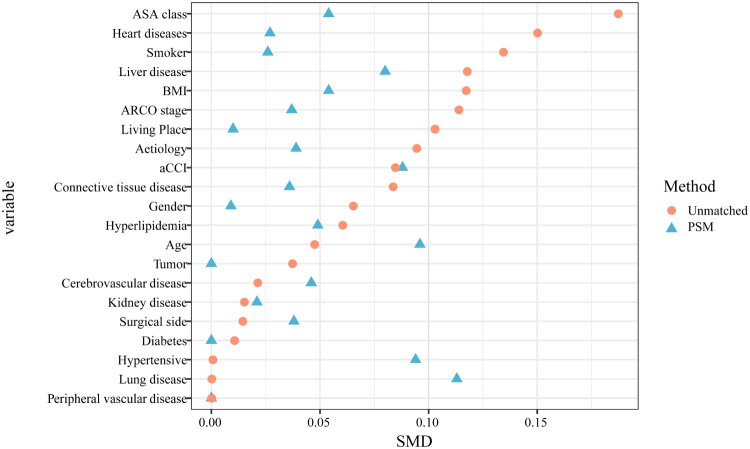
Methods: We conducted a prospective study of patients admitted to a tertiary referral hospital with osteonecrosis of the femoral head who underwent CD between October 1, 2014 and April 30, 2019, and provided a minimum 3-year follow-up assessment. Restricted cubic splines assessed the dose-effect relationship between SII and failure. Propensity score matching (PSM) balanced potential preoperative confounders. Kaplan-Meier analyses estimated cumulative incidence as a function of time for the failure between low SII and high SII groups. Multivariable Cox proportional hazards models evaluated the independent association of high SII with failure after adjustment for perioperative factors. Prespecified subgroup analyses explored heterogeneity.
Results: We found a positive relationship between the preoperative SII and failure after CD. Among 963 CD procedures performed in 676 patients, failure was observed in 97 cases in a median period of 5.4 years. The cumulative incidence of failure was 10.6% (95% CI, 8.7%, 12.8%) at 5 years. After PSM, failure rates at 5 years were identified as significant differences between the high SII and low SII groups (Log-rank p = 0.019), and that high SII was independently associated with a 1.90-fold (95% CI, 1.14, 3.18; p = 0.014) increased risk of failure. Significant heterogeneity was observed by gender and aetiology (P for interaction < 0.05).
Conclusions: Preoperative high SII is a significant risk factor for failure after CD, which could be considered when evaluating surgical indications and providing preoperative counseling to patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


