Timotius Ivan Hariyanto, Akhil Deepak Vatvani, Theo Audi Yanto
{"title":"急性心肌梗死后钠-葡萄糖共转运蛋白-2抑制剂的应用:随机试验的系统回顾、荟萃分析和荟萃回归","authors":"Timotius Ivan Hariyanto, Akhil Deepak Vatvani, Theo Audi Yanto","doi":"10.12997/jla.2025.14.3.326","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Individuals with acute myocardial infarction (AMI) face a considerable mortality risk. Recent evidence suggests that sodium-glucose cotransporter-2 inhibitors (SGLT-2i) may provide cardioprotective benefits, particularly in cases of heart failure (HF). However, the evidence regarding SGLT-2i use in AMI patients remains contradictory and ambiguous. This study investigates the efficacy and safety of SGLT-2i administration following AMI.</p><p><strong>Methods: </strong>We systematically searched Scopus, Cochrane Library, MEDLINE, and ClinicalTrials.gov for potential articles using specific keywords, with the search extending until December 15th, 2024. All published randomized controlled trials (RCTs) assessing SGLT-2i use following AMI were included. Outcomes were expressed as risk ratios (RRs) and standardized mean differences.</p><p><strong>Results: </strong>A total of 7 RCTs were included. Our pooled analysis demonstrated that SGLT-2i administration post-AMI was associated with a reduced risk of HF hospitalization (RR, 0.72; 95% confidence interval [CI], 0.60, 0.86; <i>p=</i>0.0004, I<sup>2</sup>=0%) and an improved left ventricular ejection fraction (LVEF) (SMD, 0.29; 95% CI, 0.03, 0.55; <i>p=</i>0.03; I<sup>2</sup>=60%) compared with placebo. However, there were no significant differences in all-cause mortality (<i>p</i>=0.94), cardiovascular (CV)-related mortality (<i>p</i>=0.77), stroke/transient ischemic attack (<i>p</i>=0.17), or major adverse CV events (<i>p</i>=0.16). The incidences of serious adverse events, diabetic ketoacidosis, and urinary tract infections were comparable between the 2 groups.</p><p><strong>Conclusion: </strong>The administration of SGLT-2i following AMI may reduce the risk of HF hospitalization and improve LVEF, without affecting mortality outcomes. Overall, SGLT-2i proved to be a comparatively safe treatment option.</p><p><strong>Trial registration: </strong>PROSPERO Identifier: CRD42024627125.</p>","PeriodicalId":16284,"journal":{"name":"Journal of Lipid and Atherosclerosis","volume":"14 3","pages":"326-338"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12488796/pdf/","citationCount":"0","resultStr":"{\"title\":\"Administration of Sodium-Glucose Cotransporter-2 Inhibitors Following Acute Myocardial Infarction: A Systematic Review, Meta-Analysis, and Meta-Regression of Randomized Trials.\",\"authors\":\"Timotius Ivan Hariyanto, Akhil Deepak Vatvani, Theo Audi Yanto\",\"doi\":\"10.12997/jla.2025.14.3.326\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Individuals with acute myocardial infarction (AMI) face a considerable mortality risk. Recent evidence suggests that sodium-glucose cotransporter-2 inhibitors (SGLT-2i) may provide cardioprotective benefits, particularly in cases of heart failure (HF). However, the evidence regarding SGLT-2i use in AMI patients remains contradictory and ambiguous. This study investigates the efficacy and safety of SGLT-2i administration following AMI.</p><p><strong>Methods: </strong>We systematically searched Scopus, Cochrane Library, MEDLINE, and ClinicalTrials.gov for potential articles using specific keywords, with the search extending until December 15th, 2024. All published randomized controlled trials (RCTs) assessing SGLT-2i use following AMI were included. Outcomes were expressed as risk ratios (RRs) and standardized mean differences.</p><p><strong>Results: </strong>A total of 7 RCTs were included. Our pooled analysis demonstrated that SGLT-2i administration post-AMI was associated with a reduced risk of HF hospitalization (RR, 0.72; 95% confidence interval [CI], 0.60, 0.86; <i>p=</i>0.0004, I<sup>2</sup>=0%) and an improved left ventricular ejection fraction (LVEF) (SMD, 0.29; 95% CI, 0.03, 0.55; <i>p=</i>0.03; I<sup>2</sup>=60%) compared with placebo. However, there were no significant differences in all-cause mortality (<i>p</i>=0.94), cardiovascular (CV)-related mortality (<i>p</i>=0.77), stroke/transient ischemic attack (<i>p</i>=0.17), or major adverse CV events (<i>p</i>=0.16). The incidences of serious adverse events, diabetic ketoacidosis, and urinary tract infections were comparable between the 2 groups.</p><p><strong>Conclusion: </strong>The administration of SGLT-2i following AMI may reduce the risk of HF hospitalization and improve LVEF, without affecting mortality outcomes. Overall, SGLT-2i proved to be a comparatively safe treatment option.</p><p><strong>Trial registration: </strong>PROSPERO Identifier: CRD42024627125.</p>\",\"PeriodicalId\":16284,\"journal\":{\"name\":\"Journal of Lipid and Atherosclerosis\",\"volume\":\"14 3\",\"pages\":\"326-338\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12488796/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Lipid and Atherosclerosis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12997/jla.2025.14.3.326\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Lipid and Atherosclerosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12997/jla.2025.14.3.326","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Administration of Sodium-Glucose Cotransporter-2 Inhibitors Following Acute Myocardial Infarction: A Systematic Review, Meta-Analysis, and Meta-Regression of Randomized Trials.
Objective: Individuals with acute myocardial infarction (AMI) face a considerable mortality risk. Recent evidence suggests that sodium-glucose cotransporter-2 inhibitors (SGLT-2i) may provide cardioprotective benefits, particularly in cases of heart failure (HF). However, the evidence regarding SGLT-2i use in AMI patients remains contradictory and ambiguous. This study investigates the efficacy and safety of SGLT-2i administration following AMI.
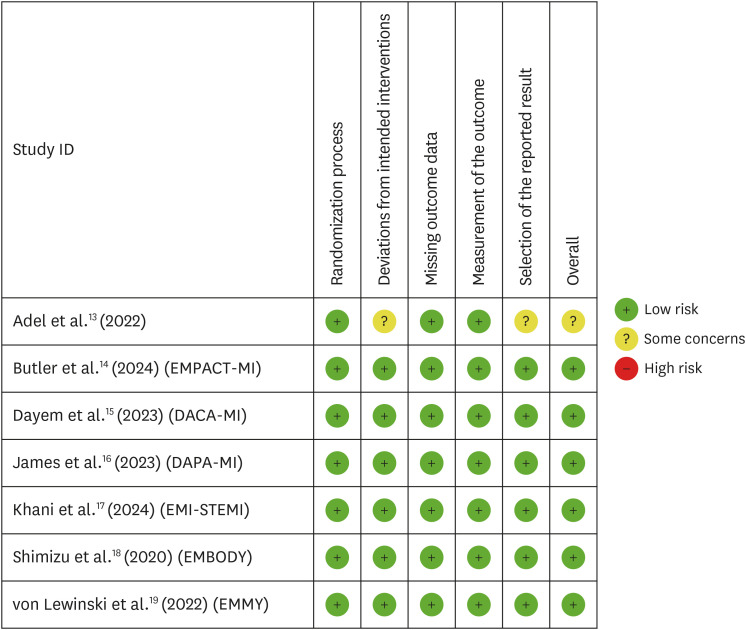
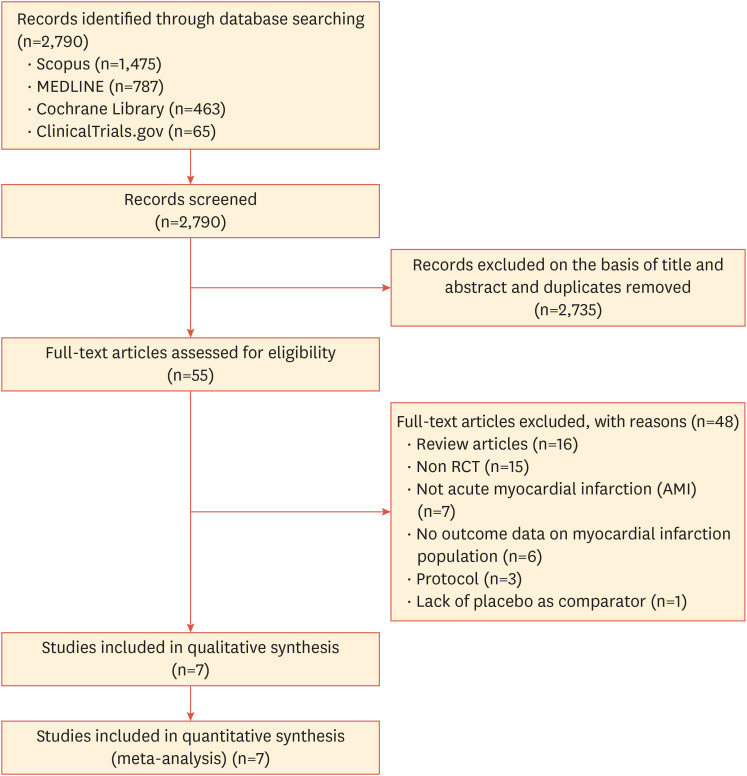
Methods: We systematically searched Scopus, Cochrane Library, MEDLINE, and ClinicalTrials.gov for potential articles using specific keywords, with the search extending until December 15th, 2024. All published randomized controlled trials (RCTs) assessing SGLT-2i use following AMI were included. Outcomes were expressed as risk ratios (RRs) and standardized mean differences.
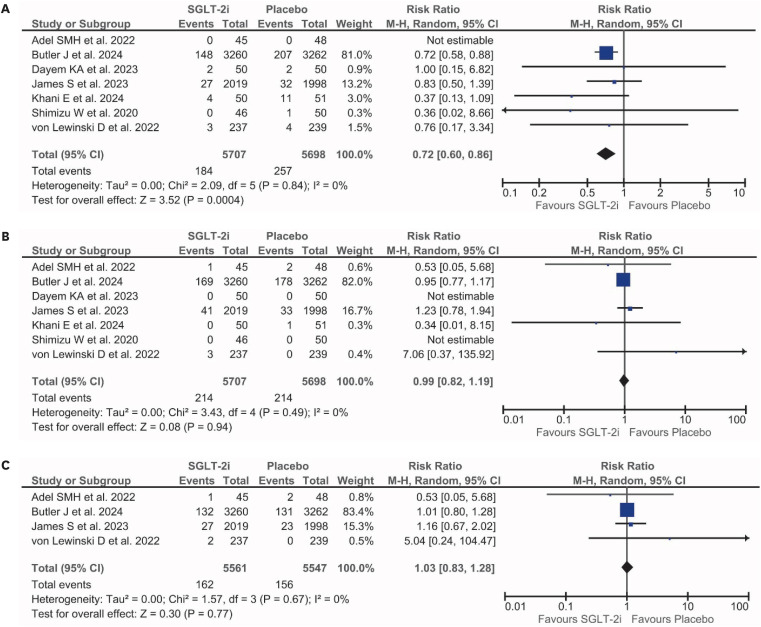
Results: A total of 7 RCTs were included. Our pooled analysis demonstrated that SGLT-2i administration post-AMI was associated with a reduced risk of HF hospitalization (RR, 0.72; 95% confidence interval [CI], 0.60, 0.86; p=0.0004, I2=0%) and an improved left ventricular ejection fraction (LVEF) (SMD, 0.29; 95% CI, 0.03, 0.55; p=0.03; I2=60%) compared with placebo. However, there were no significant differences in all-cause mortality (p=0.94), cardiovascular (CV)-related mortality (p=0.77), stroke/transient ischemic attack (p=0.17), or major adverse CV events (p=0.16). The incidences of serious adverse events, diabetic ketoacidosis, and urinary tract infections were comparable between the 2 groups.
Conclusion: The administration of SGLT-2i following AMI may reduce the risk of HF hospitalization and improve LVEF, without affecting mortality outcomes. Overall, SGLT-2i proved to be a comparatively safe treatment option.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


