{"title":"机器人辅助支气管镜定位小肺结节:一种微创手术的新方法。","authors":"Qiduo Yu, Haoshuai Yang, Jingyu Chen, Fanjia Kong, Jin Zhang, Zhoujunyi Tian, Zhenrong Zhang, Chaoyang Liang","doi":"10.3389/fsurg.2025.1641868","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Precise intraoperative localization of small pulmonary nodules is crucial for minimally invasive lung surgery. Robotic bronchoscopy, combining electromagnetic navigation and fluorescence marking, addresses limitations of traditional methods.</p><p><strong>Methods: </strong>This feasibility study included 10 patients (mean age 58) with ground-glass/partially solid nodules (mean diameter 1.42 cm). Using the Monarch® robotic system, nodules were intraoperatively marked with fluorescent dye (indocyanine green/methylene blue). Segmentectomy (4) or wedge resection (6) was performed, with lobectomy added if needed.</p><p><strong>Results: </strong>All nodules were successfully localized (mean time 16.9 min) without complications. Resected specimens confirmed central nodule placement. Pathology identified primary lung cancer in all cases: 1 adenocarcinoma <i>in situ</i>, 3 microinvasive, and 6 invasive. Lobectomy was avoided in 4 segmentectomy cases but required in 5/6 wedge resections.</p><p><strong>Conclusion: </strong>Robotic bronchoscopic localization enables safe, precise intraoperative marking, minimizing healthy tissue resection. This pilot study supports its clinical potential, warranting larger trials for validation.</p>","PeriodicalId":12564,"journal":{"name":"Frontiers in Surgery","volume":"12 ","pages":"1641868"},"PeriodicalIF":1.6000,"publicationDate":"2025-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491215/pdf/","citationCount":"0","resultStr":"{\"title\":\"Robotic-assisted bronchoscopic localization for small pulmonary nodules: a novel approach to minimally invasive surgery.\",\"authors\":\"Qiduo Yu, Haoshuai Yang, Jingyu Chen, Fanjia Kong, Jin Zhang, Zhoujunyi Tian, Zhenrong Zhang, Chaoyang Liang\",\"doi\":\"10.3389/fsurg.2025.1641868\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Precise intraoperative localization of small pulmonary nodules is crucial for minimally invasive lung surgery. Robotic bronchoscopy, combining electromagnetic navigation and fluorescence marking, addresses limitations of traditional methods.</p><p><strong>Methods: </strong>This feasibility study included 10 patients (mean age 58) with ground-glass/partially solid nodules (mean diameter 1.42 cm). Using the Monarch® robotic system, nodules were intraoperatively marked with fluorescent dye (indocyanine green/methylene blue). Segmentectomy (4) or wedge resection (6) was performed, with lobectomy added if needed.</p><p><strong>Results: </strong>All nodules were successfully localized (mean time 16.9 min) without complications. Resected specimens confirmed central nodule placement. Pathology identified primary lung cancer in all cases: 1 adenocarcinoma <i>in situ</i>, 3 microinvasive, and 6 invasive. Lobectomy was avoided in 4 segmentectomy cases but required in 5/6 wedge resections.</p><p><strong>Conclusion: </strong>Robotic bronchoscopic localization enables safe, precise intraoperative marking, minimizing healthy tissue resection. This pilot study supports its clinical potential, warranting larger trials for validation.</p>\",\"PeriodicalId\":12564,\"journal\":{\"name\":\"Frontiers in Surgery\",\"volume\":\"12 \",\"pages\":\"1641868\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491215/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fsurg.2025.1641868\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fsurg.2025.1641868","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Robotic-assisted bronchoscopic localization for small pulmonary nodules: a novel approach to minimally invasive surgery.
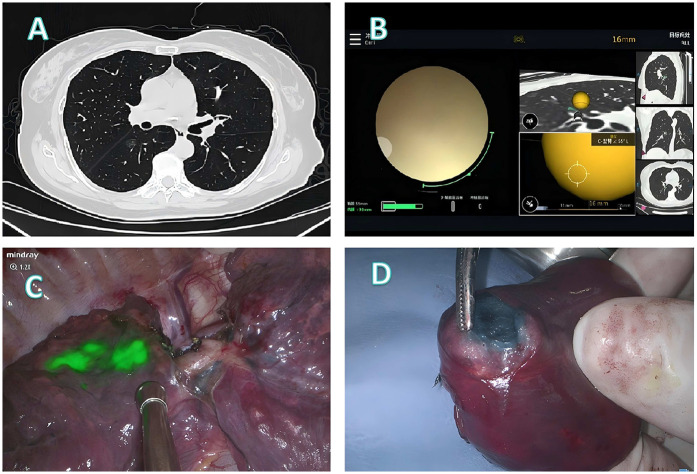
Background: Precise intraoperative localization of small pulmonary nodules is crucial for minimally invasive lung surgery. Robotic bronchoscopy, combining electromagnetic navigation and fluorescence marking, addresses limitations of traditional methods.
Methods: This feasibility study included 10 patients (mean age 58) with ground-glass/partially solid nodules (mean diameter 1.42 cm). Using the Monarch® robotic system, nodules were intraoperatively marked with fluorescent dye (indocyanine green/methylene blue). Segmentectomy (4) or wedge resection (6) was performed, with lobectomy added if needed.
Results: All nodules were successfully localized (mean time 16.9 min) without complications. Resected specimens confirmed central nodule placement. Pathology identified primary lung cancer in all cases: 1 adenocarcinoma in situ, 3 microinvasive, and 6 invasive. Lobectomy was avoided in 4 segmentectomy cases but required in 5/6 wedge resections.
Conclusion: Robotic bronchoscopic localization enables safe, precise intraoperative marking, minimizing healthy tissue resection. This pilot study supports its clinical potential, warranting larger trials for validation.
期刊介绍:
Evidence of surgical interventions go back to prehistoric times. Since then, the field of surgery has developed into a complex array of specialties and procedures, particularly with the advent of microsurgery, lasers and minimally invasive techniques. The advanced skills now required from surgeons has led to ever increasing specialization, though these still share important fundamental principles.
Frontiers in Surgery is the umbrella journal representing the publication interests of all surgical specialties. It is divided into several “Specialty Sections” listed below. All these sections have their own Specialty Chief Editor, Editorial Board and homepage, but all articles carry the citation Frontiers in Surgery.
Frontiers in Surgery calls upon medical professionals and scientists from all surgical specialties to publish their experimental and clinical studies in this journal. By assembling all surgical specialties, which nonetheless retain their independence, under the common umbrella of Frontiers in Surgery, a powerful publication venue is created. Since there is often overlap and common ground between the different surgical specialties, assembly of all surgical disciplines into a single journal will foster a collaborative dialogue amongst the surgical community. This means that publications, which are also of interest to other surgical specialties, will reach a wider audience and have greater impact.
The aim of this multidisciplinary journal is to create a discussion and knowledge platform of advances and research findings in surgical practice today to continuously improve clinical management of patients and foster innovation in this field.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


