{"title":"指南药物治疗急性心肌梗死后新发心力衰竭的效果。","authors":"Mengjie Lei, Jingyao Wang, Xiao Wang, Xue Sue, Cairong Li, Yanli Yang, Yachao Li, Zhigang Zhao, Zengming Xue","doi":"10.3389/fcvm.2025.1639213","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To investigate the impact of guideline-directed medical therapy (GDMT) during hospitalization on the prognosis of patients with heart failure (HF) episode complicating post-acute myocardial infarction (AMI).</p><p><strong>Methods: </strong>From 01/05/2017 to 30/09/2022, 527 patients with HF episode complicating post-AMI at a single medical center who were retrospectively analyzed. Based on whether GDMT during hospitalization was used in patients undergoing percutaneous coronary intervention (PCI), the patients were divided into the GDMT group (<i>n</i> = 379) and the non-GDMT group (<i>n</i> = 148), with a follow-up period of 12 months after PCI. The primary endpoint was the composite endpoint of all-cause death and all-cause readmission.</p><p><strong>Results: </strong>The incidence of the primary endpoints (7.9% vs. 18.9%, <i>P</i> < 0.001), cardiac death and cardiac readmission composite events (5.5% vs. 15.5%, <i>P</i> = 0.002), all-cause readmission events (7.1% vs. 18.9%, <i>P</i> < 0.001), and cardiac readmission events (5.0% vs. 13.5%, <i>P</i> = 0.001) in the GDMT group were lower. Cox regression analysis revealed that the incidence of primary endpoints, cardiac death and cardiac readmission composite events, all-cause readmission events, and cardiac readmission events in patients treated with GDMT during hospitalization were 0.266 times (<i>HR</i> 0.266; <i>95% CI</i> 0.146-0.487; <i>P</i> < 0.001), 0.282 times (<i>HR</i> 0.282; <i>95% CI</i> 0.137-0.581; <i>P</i> = 0.001), 0.251 times (<i>HR</i> 0.251; <i>95% CI</i> 0.136-0.464; <i>P</i> < 0.001) and 0.262 times (<i>HR</i> 0.262; <i>95% CI</i> 0.125-0.551; <i>P</i> < 0.001), respectively, compared to patients treated without GDMT.</p><p><strong>Conclusion: </strong>For patients with HF episode complicating post-AMI who undergo PCI, the use of GDMT during hospitalization reduces the incidence of primary endpoints, cardiac death and cardiac readmission composite endpoints, and all-cause readmission and cardiac readmission.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1639213"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491194/pdf/","citationCount":"0","resultStr":"{\"title\":\"The effect of guideline-directed medicine on patients with new-onset heart failure following acute myocardial infarction.\",\"authors\":\"Mengjie Lei, Jingyao Wang, Xiao Wang, Xue Sue, Cairong Li, Yanli Yang, Yachao Li, Zhigang Zhao, Zengming Xue\",\"doi\":\"10.3389/fcvm.2025.1639213\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>To investigate the impact of guideline-directed medical therapy (GDMT) during hospitalization on the prognosis of patients with heart failure (HF) episode complicating post-acute myocardial infarction (AMI).</p><p><strong>Methods: </strong>From 01/05/2017 to 30/09/2022, 527 patients with HF episode complicating post-AMI at a single medical center who were retrospectively analyzed. Based on whether GDMT during hospitalization was used in patients undergoing percutaneous coronary intervention (PCI), the patients were divided into the GDMT group (<i>n</i> = 379) and the non-GDMT group (<i>n</i> = 148), with a follow-up period of 12 months after PCI. The primary endpoint was the composite endpoint of all-cause death and all-cause readmission.</p><p><strong>Results: </strong>The incidence of the primary endpoints (7.9% vs. 18.9%, <i>P</i> < 0.001), cardiac death and cardiac readmission composite events (5.5% vs. 15.5%, <i>P</i> = 0.002), all-cause readmission events (7.1% vs. 18.9%, <i>P</i> < 0.001), and cardiac readmission events (5.0% vs. 13.5%, <i>P</i> = 0.001) in the GDMT group were lower. Cox regression analysis revealed that the incidence of primary endpoints, cardiac death and cardiac readmission composite events, all-cause readmission events, and cardiac readmission events in patients treated with GDMT during hospitalization were 0.266 times (<i>HR</i> 0.266; <i>95% CI</i> 0.146-0.487; <i>P</i> < 0.001), 0.282 times (<i>HR</i> 0.282; <i>95% CI</i> 0.137-0.581; <i>P</i> = 0.001), 0.251 times (<i>HR</i> 0.251; <i>95% CI</i> 0.136-0.464; <i>P</i> < 0.001) and 0.262 times (<i>HR</i> 0.262; <i>95% CI</i> 0.125-0.551; <i>P</i> < 0.001), respectively, compared to patients treated without GDMT.</p><p><strong>Conclusion: </strong>For patients with HF episode complicating post-AMI who undergo PCI, the use of GDMT during hospitalization reduces the incidence of primary endpoints, cardiac death and cardiac readmission composite endpoints, and all-cause readmission and cardiac readmission.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1639213\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491194/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1639213\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1639213","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:探讨住院期间指导药物治疗(GDMT)对心力衰竭(HF)发作合并急性心肌梗死(AMI)患者预后的影响。方法:回顾性分析2017年5月1日至2022年9月30日同一医疗中心527例心衰合并ami患者。根据经皮冠状动脉介入治疗(PCI)患者住院期间是否使用GDMT,将患者分为GDMT组(n = 379)和非GDMT组(n = 148), PCI术后随访12个月。主要终点为全因死亡和全因再入院的复合终点。结果:GDMT组的主要终点发生率(7.9% vs. 18.9%, P = 0.002)和全因再入院事件发生率(7.1% vs. 18.9%, P = 0.001)较低。Cox回归分析显示,住院期间接受GDMT治疗的患者主要终点、心脏死亡和心脏再入院复合事件、全因再入院事件和心脏再入院事件的发生率分别为0.266次(HR 0.266; 95% CI 0.146 ~ 0.487; P HR 0.282; 95% CI 0.137 ~ 0.581; P = 0.001)、0.251次(HR 0.251; 95% CI 0.136 ~ 0.464; P HR 0.262; 95% CI 0.125 ~ 0.551;结论:对于心衰合并ami后行PCI的患者,住院期间使用GDMT可降低主要终点、心源性死亡和心脏再入院复合终点以及全因再入院和心脏再入院的发生率。
The effect of guideline-directed medicine on patients with new-onset heart failure following acute myocardial infarction.
Aims: To investigate the impact of guideline-directed medical therapy (GDMT) during hospitalization on the prognosis of patients with heart failure (HF) episode complicating post-acute myocardial infarction (AMI).
Methods: From 01/05/2017 to 30/09/2022, 527 patients with HF episode complicating post-AMI at a single medical center who were retrospectively analyzed. Based on whether GDMT during hospitalization was used in patients undergoing percutaneous coronary intervention (PCI), the patients were divided into the GDMT group (n = 379) and the non-GDMT group (n = 148), with a follow-up period of 12 months after PCI. The primary endpoint was the composite endpoint of all-cause death and all-cause readmission.
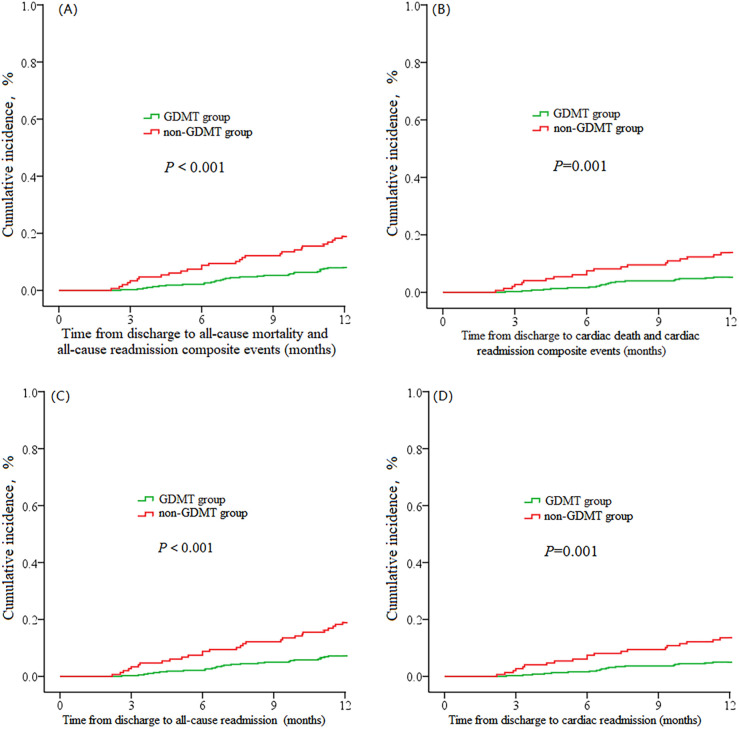
Results: The incidence of the primary endpoints (7.9% vs. 18.9%, P < 0.001), cardiac death and cardiac readmission composite events (5.5% vs. 15.5%, P = 0.002), all-cause readmission events (7.1% vs. 18.9%, P < 0.001), and cardiac readmission events (5.0% vs. 13.5%, P = 0.001) in the GDMT group were lower. Cox regression analysis revealed that the incidence of primary endpoints, cardiac death and cardiac readmission composite events, all-cause readmission events, and cardiac readmission events in patients treated with GDMT during hospitalization were 0.266 times (HR 0.266; 95% CI 0.146-0.487; P < 0.001), 0.282 times (HR 0.282; 95% CI 0.137-0.581; P = 0.001), 0.251 times (HR 0.251; 95% CI 0.136-0.464; P < 0.001) and 0.262 times (HR 0.262; 95% CI 0.125-0.551; P < 0.001), respectively, compared to patients treated without GDMT.
Conclusion: For patients with HF episode complicating post-AMI who undergo PCI, the use of GDMT during hospitalization reduces the incidence of primary endpoints, cardiac death and cardiac readmission composite endpoints, and all-cause readmission and cardiac readmission.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


