{"title":"新生儿ABO溶血性疾病使用IVIG的时机。","authors":"Na Ma, Feihong Zhang, Yong Hu, Bin Xia","doi":"10.1186/s12887-025-06062-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>ABO hemolytic disease of the newborn (ABO HDN) is the most prevalent cause of hemolytic disease of the newborn, often leading to hyperbilirubinemia. In some cases, ABO HDN can progress to significant hyperbilirubinemia. The role of intravenous immunoglobulin (IVIG) in treating ABO HDN remains controversial. Several key questions regarding significant hyperbilirubinemia remain unanswered: What are the risk factors of ABO HDN with significant hyperbilirubinemia? Can IVIG provide benefits for ABO HDN with significant hyperbilirubinemia? Where do we place IVIG in the treatment sequence paradigm of ABO HDN? How do we best stratify ABO HDN with significant hyperbilirubinemia for IVIG therapy?</p><p><strong>Methods: </strong>We conducted a retrospective cohort study include 948 newborns from West China Second University Hospital, divided into two groups according to the use/nonuse of IVIG. The maternal and neonatal baseline clinical data were collected from digital medical record system. The risk factors of the significant hyperbilirubinemia associated with ABO HDN were investigated using univariate and multivariate analysis. The generalized additive mixed model (GAMM) was used to analyze the nonlinear relationship of bilirubin level with different treatment over time.</p><p><strong>Results: </strong>A total of 948 newborns fulfilled the inclusion criteria, with 143 (15.1%) in the IVIG group, and 805 (84.9%) in the non-IVIG group. (1) The multivariate analysis found that gestational age ≥ 37 weeks (OR 4.19; p = 0.019), age at admission range 24-48 h (OR 9.69; p = 0.03) and age at admission >48 h (OR 50.31; p < 0.0001) were affect significant hyperbilirubinemia in neonates. (2) The total serum bilirubin (TSB) descent speed of IVIG group (0.69µmol/L/h, 95%CI, 0.48-0.89µmol/L/h) was higher than non-IVIG group (0.21µmol/L/h, 95%CI, 0.14-0.29µmol/L/h) among the neonates with age at admission ≤ 48 h (p < 0.0001);No adverse effects related to IVIG treatment were recorded in either group.</p><p><strong>Conclusion: </strong>Regular monitoring of TSB levels starting 24 h after birth is an effective strategy to prevent severe hyperbilirubinemia in ABO HDN. For southwest Chinese neonates, IVIG should not be routinely used to treat ABO HDN in those admitted > 48 h after birth.</p>","PeriodicalId":9144,"journal":{"name":"BMC Pediatrics","volume":"25 1","pages":"731"},"PeriodicalIF":2.0000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12492713/pdf/","citationCount":"0","resultStr":"{\"title\":\"The timing of using IVIG for neonatal ABO hemolytic disease.\",\"authors\":\"Na Ma, Feihong Zhang, Yong Hu, Bin Xia\",\"doi\":\"10.1186/s12887-025-06062-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>ABO hemolytic disease of the newborn (ABO HDN) is the most prevalent cause of hemolytic disease of the newborn, often leading to hyperbilirubinemia. In some cases, ABO HDN can progress to significant hyperbilirubinemia. The role of intravenous immunoglobulin (IVIG) in treating ABO HDN remains controversial. Several key questions regarding significant hyperbilirubinemia remain unanswered: What are the risk factors of ABO HDN with significant hyperbilirubinemia? Can IVIG provide benefits for ABO HDN with significant hyperbilirubinemia? Where do we place IVIG in the treatment sequence paradigm of ABO HDN? How do we best stratify ABO HDN with significant hyperbilirubinemia for IVIG therapy?</p><p><strong>Methods: </strong>We conducted a retrospective cohort study include 948 newborns from West China Second University Hospital, divided into two groups according to the use/nonuse of IVIG. The maternal and neonatal baseline clinical data were collected from digital medical record system. The risk factors of the significant hyperbilirubinemia associated with ABO HDN were investigated using univariate and multivariate analysis. The generalized additive mixed model (GAMM) was used to analyze the nonlinear relationship of bilirubin level with different treatment over time.</p><p><strong>Results: </strong>A total of 948 newborns fulfilled the inclusion criteria, with 143 (15.1%) in the IVIG group, and 805 (84.9%) in the non-IVIG group. (1) The multivariate analysis found that gestational age ≥ 37 weeks (OR 4.19; p = 0.019), age at admission range 24-48 h (OR 9.69; p = 0.03) and age at admission >48 h (OR 50.31; p < 0.0001) were affect significant hyperbilirubinemia in neonates. (2) The total serum bilirubin (TSB) descent speed of IVIG group (0.69µmol/L/h, 95%CI, 0.48-0.89µmol/L/h) was higher than non-IVIG group (0.21µmol/L/h, 95%CI, 0.14-0.29µmol/L/h) among the neonates with age at admission ≤ 48 h (p < 0.0001);No adverse effects related to IVIG treatment were recorded in either group.</p><p><strong>Conclusion: </strong>Regular monitoring of TSB levels starting 24 h after birth is an effective strategy to prevent severe hyperbilirubinemia in ABO HDN. For southwest Chinese neonates, IVIG should not be routinely used to treat ABO HDN in those admitted > 48 h after birth.</p>\",\"PeriodicalId\":9144,\"journal\":{\"name\":\"BMC Pediatrics\",\"volume\":\"25 1\",\"pages\":\"731\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-10-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12492713/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12887-025-06062-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12887-025-06062-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:ABO新生儿溶血性疾病(ABO HDN)是新生儿溶血性疾病最常见的病因,常导致高胆红素血症。在某些情况下,ABO HDN可发展为显著的高胆红素血症。静脉注射免疫球蛋白(IVIG)在治疗ABO HDN中的作用仍然存在争议。关于显著高胆红素血症的几个关键问题仍未得到解答:ABO HDN伴显著高胆红素血症的危险因素是什么?IVIG能对ABO HDN伴显著高胆红素血症提供益处吗?在ABO HDN的治疗顺序范例中,我们将IVIG置于何处?我们如何最好地将ABO HDN与显著高胆红素血症进行IVIG治疗?方法:对华西第二大学附属医院948例新生儿进行回顾性队列研究,按是否使用IVIG分为两组。从数字病案系统中收集产妇和新生儿的基线临床资料。采用单因素和多因素分析探讨ABO HDN相关的显著高胆红素血症的危险因素。采用广义加性混合模型(GAMM)分析了不同处理下胆红素水平随时间的非线性关系。结果:948例新生儿符合纳入标准,IVIG组143例(15.1%),非IVIG组805例(84.9%)。(1)多因素分析发现,胎龄≥37周(OR 4.19, p = 0.019)、出生时年龄24 ~ 48 h (OR 9.69, p = 0.03)、出生时年龄bb0 ~ 48 h (OR 50.31; p)。结论:出生后24 h开始定期监测TSB水平是预防ABO HDN严重高胆红素血症的有效策略。对于中国西南地区的新生儿,出生后48小时入院的新生儿,不应常规使用IVIG治疗ABO HDN。
The timing of using IVIG for neonatal ABO hemolytic disease.
Background: ABO hemolytic disease of the newborn (ABO HDN) is the most prevalent cause of hemolytic disease of the newborn, often leading to hyperbilirubinemia. In some cases, ABO HDN can progress to significant hyperbilirubinemia. The role of intravenous immunoglobulin (IVIG) in treating ABO HDN remains controversial. Several key questions regarding significant hyperbilirubinemia remain unanswered: What are the risk factors of ABO HDN with significant hyperbilirubinemia? Can IVIG provide benefits for ABO HDN with significant hyperbilirubinemia? Where do we place IVIG in the treatment sequence paradigm of ABO HDN? How do we best stratify ABO HDN with significant hyperbilirubinemia for IVIG therapy?
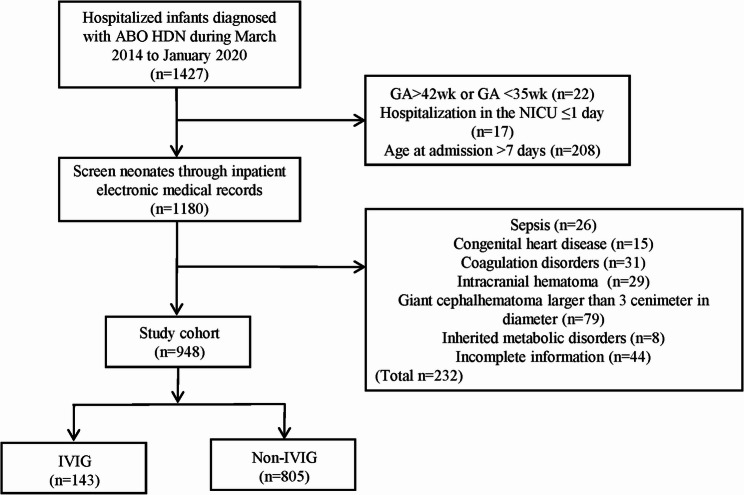
Methods: We conducted a retrospective cohort study include 948 newborns from West China Second University Hospital, divided into two groups according to the use/nonuse of IVIG. The maternal and neonatal baseline clinical data were collected from digital medical record system. The risk factors of the significant hyperbilirubinemia associated with ABO HDN were investigated using univariate and multivariate analysis. The generalized additive mixed model (GAMM) was used to analyze the nonlinear relationship of bilirubin level with different treatment over time.
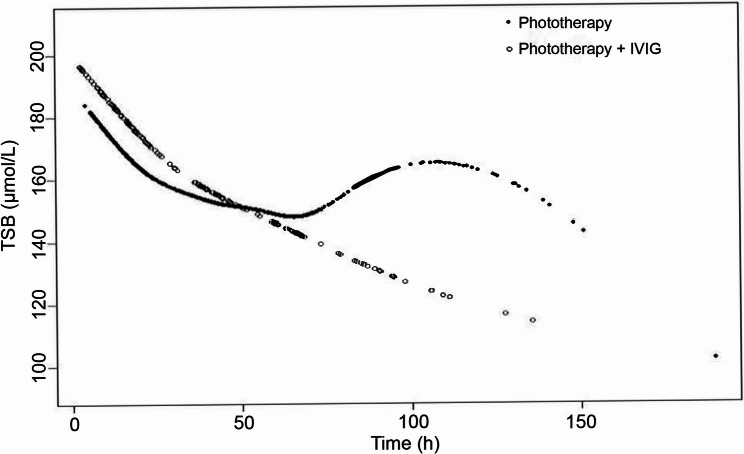
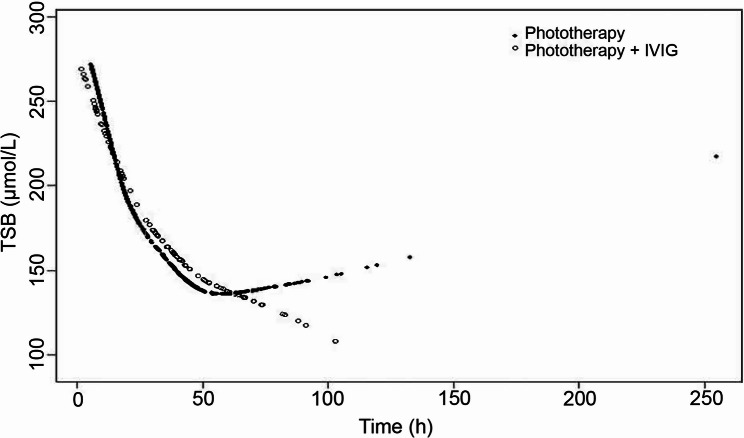
Results: A total of 948 newborns fulfilled the inclusion criteria, with 143 (15.1%) in the IVIG group, and 805 (84.9%) in the non-IVIG group. (1) The multivariate analysis found that gestational age ≥ 37 weeks (OR 4.19; p = 0.019), age at admission range 24-48 h (OR 9.69; p = 0.03) and age at admission >48 h (OR 50.31; p < 0.0001) were affect significant hyperbilirubinemia in neonates. (2) The total serum bilirubin (TSB) descent speed of IVIG group (0.69µmol/L/h, 95%CI, 0.48-0.89µmol/L/h) was higher than non-IVIG group (0.21µmol/L/h, 95%CI, 0.14-0.29µmol/L/h) among the neonates with age at admission ≤ 48 h (p < 0.0001);No adverse effects related to IVIG treatment were recorded in either group.
Conclusion: Regular monitoring of TSB levels starting 24 h after birth is an effective strategy to prevent severe hyperbilirubinemia in ABO HDN. For southwest Chinese neonates, IVIG should not be routinely used to treat ABO HDN in those admitted > 48 h after birth.
期刊介绍:
BMC Pediatrics is an open access journal publishing peer-reviewed research articles in all aspects of health care in neonates, children and adolescents, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


