Jazmine M Li, Dawn Gruss, Timothy Hunt, James David, Emma Rodgers, Nabila El-Bassel, Bruce R Schackman, Laura E Starbird
{"title":"实施循证做法以减少纽约州社区阿片类药物过量死亡的成本。","authors":"Jazmine M Li, Dawn Gruss, Timothy Hunt, James David, Emma Rodgers, Nabila El-Bassel, Bruce R Schackman, Laura E Starbird","doi":"10.1186/s13722-025-00606-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The HEALing Communities Study was a multi-site cluster randomized waitlist-controlled trial evaluating a community-engaged, data-driven intervention to select and deploy evidence-based practices (EBPs) including overdose education and naloxone distribution (OEND), medication for opioid use disorder (MOUD), and safer opioid prescribing. The trial was conducted in 67 highly impacted communities in 4 states, including 8 Rural and 8 urban communities in New York State (NYS). To inform future community-level decision making, we estimated the implementation costs of the EBPs selected by NYS communities.</p><p><strong>Methods: </strong>The study was implemented between January 2020-June 2022 (Wave 1, 30 months duration including the peak COVID-19 emergency period) and July 2022-December 2023 (Wave 2, 18 months); each wave included 4 Rural and 4 urban NYS communities. We collected cost data prospectively using invoices, administrative records, and interviews with program staff and stakeholders. We then conducted a micro-costing analysis from the community perspective and compared costs from Waves 1 and 2.</p><p><strong>Results: </strong>In both Waves, each community deployed on average 15 EBPs (range 8-25). EBP costs averaged $705,000 (range $320,000-$1.3 million) and $312,000 (range $39,200-$686,300) in Waves 1 and 2, respectively. In Wave 1, 25% of costs were allocated for OEND, 71% for MOUD, and 4% for safer prescribing, compared to 38% for OEND, 60% for MOUD, and 2% for safer prescribing in Wave 2. Average EBP costs per community were $147,600 (range $20,900-$374,000) for those in the OEND category, $345,400 (range $4,100-$1.1 million) for MOUD, and $16,400 (range $360-$105,500) for safer prescribing. Total EBP cost per capita in urban communities was $0.32 compared to $2.65 in Rural communities in Wave 1, and $0.41 urban communities compared to $0.65 in Rural communities in Wave 2.</p><p><strong>Conclusions: </strong>The lower EBP costs in Wave 2 resulted from differences in EBP categories and specific EBPs selected and may also reflect differences in the duration of the intervention and the impact of the COVID-19 pandemic over time. Higher per capita costs in rural communities indicate that many costs were not directly related to the number of individuals served.</p>","PeriodicalId":54223,"journal":{"name":"Addiction Science & Clinical Practice","volume":"20 1","pages":"77"},"PeriodicalIF":3.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12486734/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost of implementing evidence-based practices to reduce opioid overdose fatalities in New York State communities.\",\"authors\":\"Jazmine M Li, Dawn Gruss, Timothy Hunt, James David, Emma Rodgers, Nabila El-Bassel, Bruce R Schackman, Laura E Starbird\",\"doi\":\"10.1186/s13722-025-00606-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The HEALing Communities Study was a multi-site cluster randomized waitlist-controlled trial evaluating a community-engaged, data-driven intervention to select and deploy evidence-based practices (EBPs) including overdose education and naloxone distribution (OEND), medication for opioid use disorder (MOUD), and safer opioid prescribing. The trial was conducted in 67 highly impacted communities in 4 states, including 8 Rural and 8 urban communities in New York State (NYS). To inform future community-level decision making, we estimated the implementation costs of the EBPs selected by NYS communities.</p><p><strong>Methods: </strong>The study was implemented between January 2020-June 2022 (Wave 1, 30 months duration including the peak COVID-19 emergency period) and July 2022-December 2023 (Wave 2, 18 months); each wave included 4 Rural and 4 urban NYS communities. We collected cost data prospectively using invoices, administrative records, and interviews with program staff and stakeholders. We then conducted a micro-costing analysis from the community perspective and compared costs from Waves 1 and 2.</p><p><strong>Results: </strong>In both Waves, each community deployed on average 15 EBPs (range 8-25). EBP costs averaged $705,000 (range $320,000-$1.3 million) and $312,000 (range $39,200-$686,300) in Waves 1 and 2, respectively. In Wave 1, 25% of costs were allocated for OEND, 71% for MOUD, and 4% for safer prescribing, compared to 38% for OEND, 60% for MOUD, and 2% for safer prescribing in Wave 2. Average EBP costs per community were $147,600 (range $20,900-$374,000) for those in the OEND category, $345,400 (range $4,100-$1.1 million) for MOUD, and $16,400 (range $360-$105,500) for safer prescribing. Total EBP cost per capita in urban communities was $0.32 compared to $2.65 in Rural communities in Wave 1, and $0.41 urban communities compared to $0.65 in Rural communities in Wave 2.</p><p><strong>Conclusions: </strong>The lower EBP costs in Wave 2 resulted from differences in EBP categories and specific EBPs selected and may also reflect differences in the duration of the intervention and the impact of the COVID-19 pandemic over time. Higher per capita costs in rural communities indicate that many costs were not directly related to the number of individuals served.</p>\",\"PeriodicalId\":54223,\"journal\":{\"name\":\"Addiction Science & Clinical Practice\",\"volume\":\"20 1\",\"pages\":\"77\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12486734/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Addiction Science & Clinical Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13722-025-00606-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SUBSTANCE ABUSE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Addiction Science & Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13722-025-00606-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
Cost of implementing evidence-based practices to reduce opioid overdose fatalities in New York State communities.
Background: The HEALing Communities Study was a multi-site cluster randomized waitlist-controlled trial evaluating a community-engaged, data-driven intervention to select and deploy evidence-based practices (EBPs) including overdose education and naloxone distribution (OEND), medication for opioid use disorder (MOUD), and safer opioid prescribing. The trial was conducted in 67 highly impacted communities in 4 states, including 8 Rural and 8 urban communities in New York State (NYS). To inform future community-level decision making, we estimated the implementation costs of the EBPs selected by NYS communities.
Methods: The study was implemented between January 2020-June 2022 (Wave 1, 30 months duration including the peak COVID-19 emergency period) and July 2022-December 2023 (Wave 2, 18 months); each wave included 4 Rural and 4 urban NYS communities. We collected cost data prospectively using invoices, administrative records, and interviews with program staff and stakeholders. We then conducted a micro-costing analysis from the community perspective and compared costs from Waves 1 and 2.
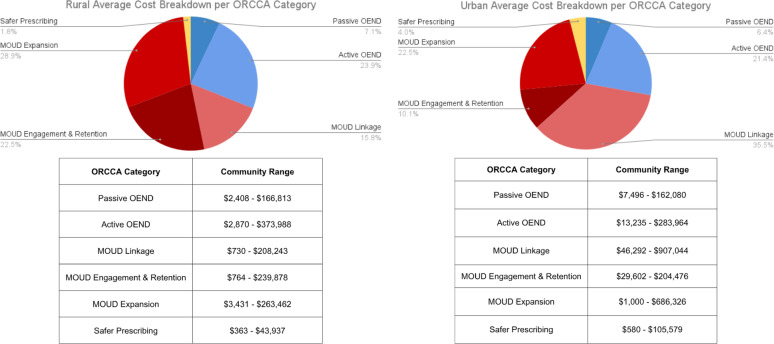
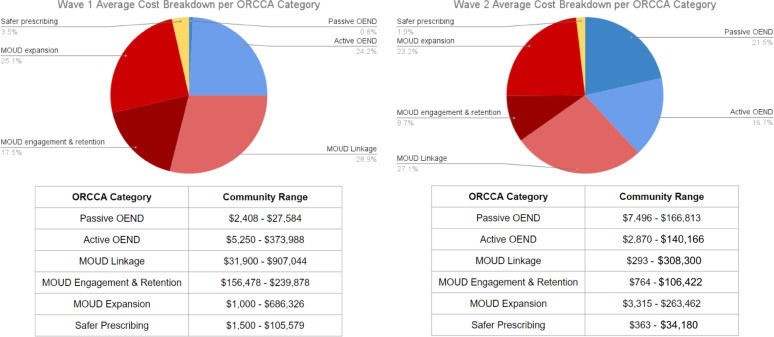
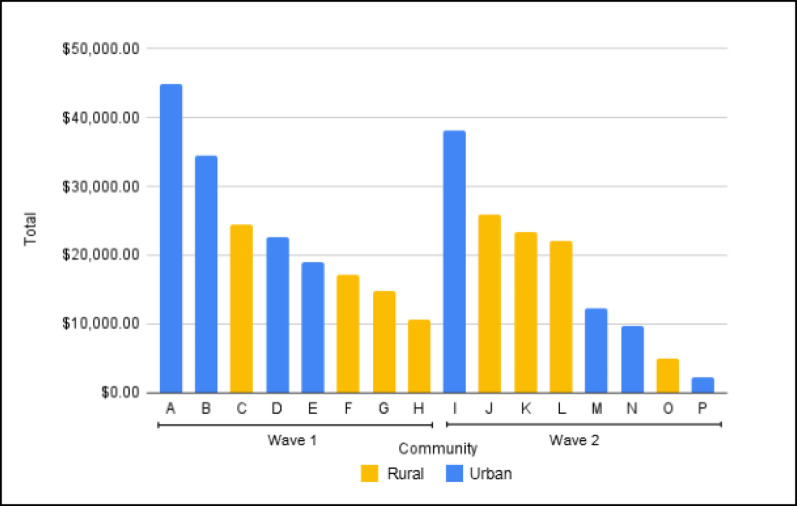
Results: In both Waves, each community deployed on average 15 EBPs (range 8-25). EBP costs averaged $705,000 (range $320,000-$1.3 million) and $312,000 (range $39,200-$686,300) in Waves 1 and 2, respectively. In Wave 1, 25% of costs were allocated for OEND, 71% for MOUD, and 4% for safer prescribing, compared to 38% for OEND, 60% for MOUD, and 2% for safer prescribing in Wave 2. Average EBP costs per community were $147,600 (range $20,900-$374,000) for those in the OEND category, $345,400 (range $4,100-$1.1 million) for MOUD, and $16,400 (range $360-$105,500) for safer prescribing. Total EBP cost per capita in urban communities was $0.32 compared to $2.65 in Rural communities in Wave 1, and $0.41 urban communities compared to $0.65 in Rural communities in Wave 2.
Conclusions: The lower EBP costs in Wave 2 resulted from differences in EBP categories and specific EBPs selected and may also reflect differences in the duration of the intervention and the impact of the COVID-19 pandemic over time. Higher per capita costs in rural communities indicate that many costs were not directly related to the number of individuals served.
期刊介绍:
Addiction Science & Clinical Practice provides a forum for clinically relevant research and perspectives that contribute to improving the quality of care for people with unhealthy alcohol, tobacco, or other drug use and addictive behaviours across a spectrum of clinical settings.
Addiction Science & Clinical Practice accepts articles of clinical relevance related to the prevention and treatment of unhealthy alcohol, tobacco, and other drug use across the spectrum of clinical settings. Topics of interest address issues related to the following: the spectrum of unhealthy use of alcohol, tobacco, and other drugs among the range of affected persons (e.g., not limited by age, race/ethnicity, gender, or sexual orientation); the array of clinical prevention and treatment practices (from health messages, to identification and early intervention, to more extensive interventions including counseling and pharmacotherapy and other management strategies); and identification and management of medical, psychiatric, social, and other health consequences of substance use.
Addiction Science & Clinical Practice is particularly interested in articles that address how to improve the quality of care for people with unhealthy substance use and related conditions as described in the (US) Institute of Medicine report, Improving the Quality of Healthcare for Mental Health and Substance Use Conditions (Washington, DC: National Academies Press, 2006). Such articles address the quality of care and of health services. Although the journal also welcomes submissions that address these conditions in addiction speciality-treatment settings, the journal is particularly interested in including articles that address unhealthy use outside these settings, including experience with novel models of care and outcomes, and outcomes of research-practice collaborations.
Although Addiction Science & Clinical Practice is generally not an outlet for basic science research, we will accept basic science research manuscripts that have clearly described potential clinical relevance and are accessible to audiences outside a narrow laboratory research field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


