Danyal Bakht, Maaz Amir, Fahad Saleem, Ahmed Asif, Mohammad Maheer Mubashir, Abdullah Shahid Farooq, Muhammad Zauraiz Malik, Ahmad Hassan, Kinza Bakht, Muhammad Arham, Syed Faqeer Hussain Bokhari, Muhammad Numan Awais, Muhammad Khan Buhadur Ali, Allah Dad, Muhammad Rizwan Akram
{"title":"系统回顾和荟萃分析:手术心脏去神经支配对术后房颤有效吗?","authors":"Danyal Bakht, Maaz Amir, Fahad Saleem, Ahmed Asif, Mohammad Maheer Mubashir, Abdullah Shahid Farooq, Muhammad Zauraiz Malik, Ahmad Hassan, Kinza Bakht, Muhammad Arham, Syed Faqeer Hussain Bokhari, Muhammad Numan Awais, Muhammad Khan Buhadur Ali, Allah Dad, Muhammad Rizwan Akram","doi":"10.4330/wjc.v17.i9.110756","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postoperative atrial fibrillation (POAF) is a complication after cardiac surgeries associated with increased morbidity and hospital stay. Surgical cardiac denervation, which reduces autonomic input to the heart, has been proposed as a good preventive against POAF. However, evidence on its effectiveness remains inconsistent.</p><p><strong>Aim: </strong>To evaluate the impact of surgical cardiac denervation on the incidence of POAF and related clinical outcomes.</p><p><strong>Methods: </strong>This meta-analysis adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A literature search was conducted across PubMed, Cochrane, ScienceDirect, and EMBASE up to April 2025 using a preformed search strategy using Medical Subject Headings terms and free-text keywords. Risk of bias assessment was done <i>via</i> Risk of Bias 2.0 and Risk Of Bias In Non-randomized Studies - of Interventions tools. Study analysis was performed using Review Manager version 5.4, with heterogeneity assessed <i>via I</i> <sup>2</sup> values and appropriate fixed- or random-effects models applied.</p><p><strong>Results: </strong>Five studies (<i>N</i> = 1266) were included, with 627 patients undergoing cardiac denervation and 639 serving as controls. Denervation did not significantly reduce overall POAF [odds ratio = 0.71; 95% confidence interval (CI): 0.32-1.58; <i>P</i> = 0.40; <i>I</i> <sup>2</sup> = 83%], but was associated with a significant reduction in persistent atrial fibrillation (odds ratio = 0.19; 95%CI: 0.10-0.36; <i>P</i> < 0.00001; <i>I</i> <sup>2</sup> = 0%). Among secondary outcomes, only postoperative serum magnesium levels significantly reduced the denervation group (mean difference: -0.07 mmol/L; 95%CI: -0.08 to -0.06; <i>P</i> < 0.00001). Other outcomes, such as reoperation for bleeding, stroke/transient ischemic attack, length of hospital stay, 30-day mortality, and postoperative drainage, did not show any significant difference.</p><p><strong>Conclusion: </strong>Surgical cardiac denervation does not significantly reduce overall POAF but does lower the incidence of persistent atrial fibrillation. It is also shown to decrease serum magnesium levels. Other outcomes, such as stroke, reoperation, and hospital stay, showed no significant differences.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 9","pages":"110756"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476607/pdf/","citationCount":"0","resultStr":"{\"title\":\"Systematic review and meta-analysis: Is surgical cardiac denervation effective against postoperative atrial fibrillation?\",\"authors\":\"Danyal Bakht, Maaz Amir, Fahad Saleem, Ahmed Asif, Mohammad Maheer Mubashir, Abdullah Shahid Farooq, Muhammad Zauraiz Malik, Ahmad Hassan, Kinza Bakht, Muhammad Arham, Syed Faqeer Hussain Bokhari, Muhammad Numan Awais, Muhammad Khan Buhadur Ali, Allah Dad, Muhammad Rizwan Akram\",\"doi\":\"10.4330/wjc.v17.i9.110756\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Postoperative atrial fibrillation (POAF) is a complication after cardiac surgeries associated with increased morbidity and hospital stay. Surgical cardiac denervation, which reduces autonomic input to the heart, has been proposed as a good preventive against POAF. However, evidence on its effectiveness remains inconsistent.</p><p><strong>Aim: </strong>To evaluate the impact of surgical cardiac denervation on the incidence of POAF and related clinical outcomes.</p><p><strong>Methods: </strong>This meta-analysis adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A literature search was conducted across PubMed, Cochrane, ScienceDirect, and EMBASE up to April 2025 using a preformed search strategy using Medical Subject Headings terms and free-text keywords. Risk of bias assessment was done <i>via</i> Risk of Bias 2.0 and Risk Of Bias In Non-randomized Studies - of Interventions tools. Study analysis was performed using Review Manager version 5.4, with heterogeneity assessed <i>via I</i> <sup>2</sup> values and appropriate fixed- or random-effects models applied.</p><p><strong>Results: </strong>Five studies (<i>N</i> = 1266) were included, with 627 patients undergoing cardiac denervation and 639 serving as controls. Denervation did not significantly reduce overall POAF [odds ratio = 0.71; 95% confidence interval (CI): 0.32-1.58; <i>P</i> = 0.40; <i>I</i> <sup>2</sup> = 83%], but was associated with a significant reduction in persistent atrial fibrillation (odds ratio = 0.19; 95%CI: 0.10-0.36; <i>P</i> < 0.00001; <i>I</i> <sup>2</sup> = 0%). Among secondary outcomes, only postoperative serum magnesium levels significantly reduced the denervation group (mean difference: -0.07 mmol/L; 95%CI: -0.08 to -0.06; <i>P</i> < 0.00001). Other outcomes, such as reoperation for bleeding, stroke/transient ischemic attack, length of hospital stay, 30-day mortality, and postoperative drainage, did not show any significant difference.</p><p><strong>Conclusion: </strong>Surgical cardiac denervation does not significantly reduce overall POAF but does lower the incidence of persistent atrial fibrillation. It is also shown to decrease serum magnesium levels. Other outcomes, such as stroke, reoperation, and hospital stay, showed no significant differences.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"17 9\",\"pages\":\"110756\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476607/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v17.i9.110756\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i9.110756","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:术后心房颤动(POAF)是心脏手术后的并发症,与发病率和住院时间增加有关。外科心脏去神经,减少自主神经输入心脏,已被提出作为一个很好的预防POAF。然而,关于其有效性的证据仍然不一致。目的:探讨外科心脏去神经支配对POAF发生率及相关临床结局的影响。方法:本荟萃分析遵循系统评价和荟萃分析指南的首选报告项目。文献检索在PubMed、Cochrane、ScienceDirect和EMBASE上进行,截止到2025年4月,使用预先制定的搜索策略,使用医学主题词和自由文本关键词。偏倚风险评估通过Risk of bias 2.0和Risk of bias In non -random Studies - of Interventions工具完成。使用Review Manager版本5.4进行研究分析,通过i2值评估异质性,并应用适当的固定或随机效应模型。结果:纳入5项研究(N = 1266), 627例患者接受心脏去神经支配,639例作为对照。去神经治疗没有显著降低POAF[优势比= 0.71;95%置信区间(CI): 0.32-1.58;P = 0.40;i2 = 83%],但与持续性房颤的显著降低相关(优势比= 0.19;95%CI: 0.10-0.36; P < 0.00001; i2 = 0%)。在次要结局中,只有术后血清镁水平显著降低去神经组(平均差异:-0.07 mmol/L; 95%CI: -0.08 ~ -0.06; P < 0.00001)。其他结果,如因出血而再次手术、卒中/短暂性脑缺血发作、住院时间、30天死亡率和术后引流,均无显著差异。结论:手术心脏去神经不能显著降低总POAF,但可以降低持续性心房颤动的发生率。它也被证明可以降低血清镁水平。其他结果,如中风、再手术和住院时间,没有显着差异。
Systematic review and meta-analysis: Is surgical cardiac denervation effective against postoperative atrial fibrillation?
Background: Postoperative atrial fibrillation (POAF) is a complication after cardiac surgeries associated with increased morbidity and hospital stay. Surgical cardiac denervation, which reduces autonomic input to the heart, has been proposed as a good preventive against POAF. However, evidence on its effectiveness remains inconsistent.
Aim: To evaluate the impact of surgical cardiac denervation on the incidence of POAF and related clinical outcomes.
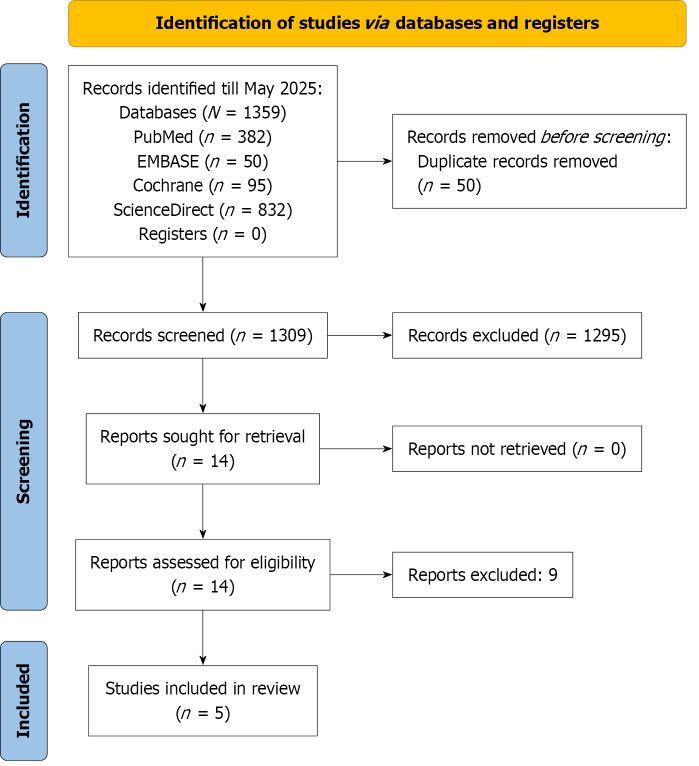
Methods: This meta-analysis adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A literature search was conducted across PubMed, Cochrane, ScienceDirect, and EMBASE up to April 2025 using a preformed search strategy using Medical Subject Headings terms and free-text keywords. Risk of bias assessment was done via Risk of Bias 2.0 and Risk Of Bias In Non-randomized Studies - of Interventions tools. Study analysis was performed using Review Manager version 5.4, with heterogeneity assessed via I2 values and appropriate fixed- or random-effects models applied.
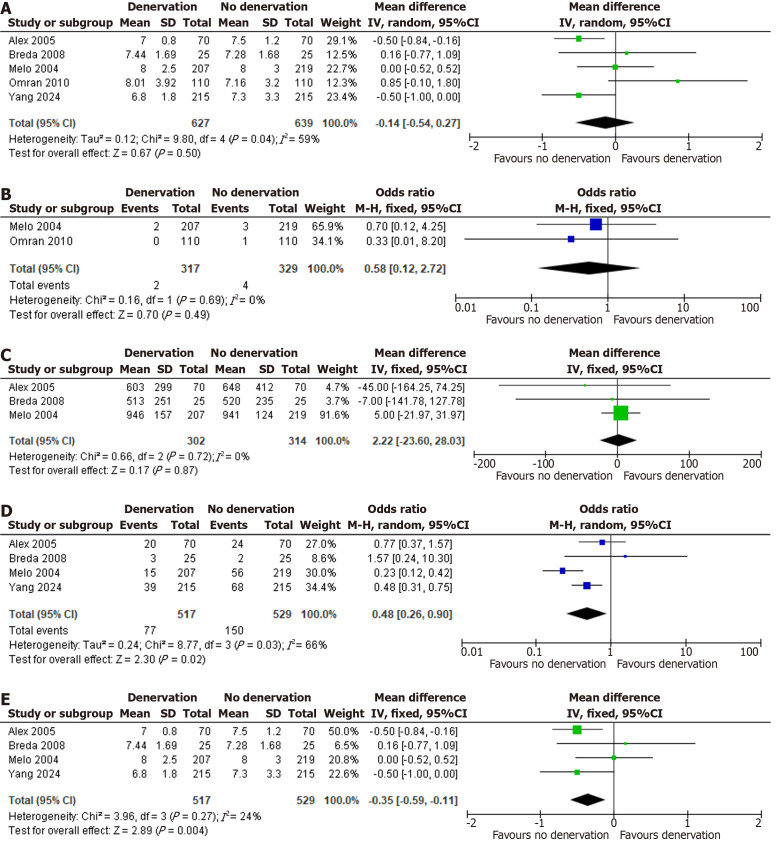
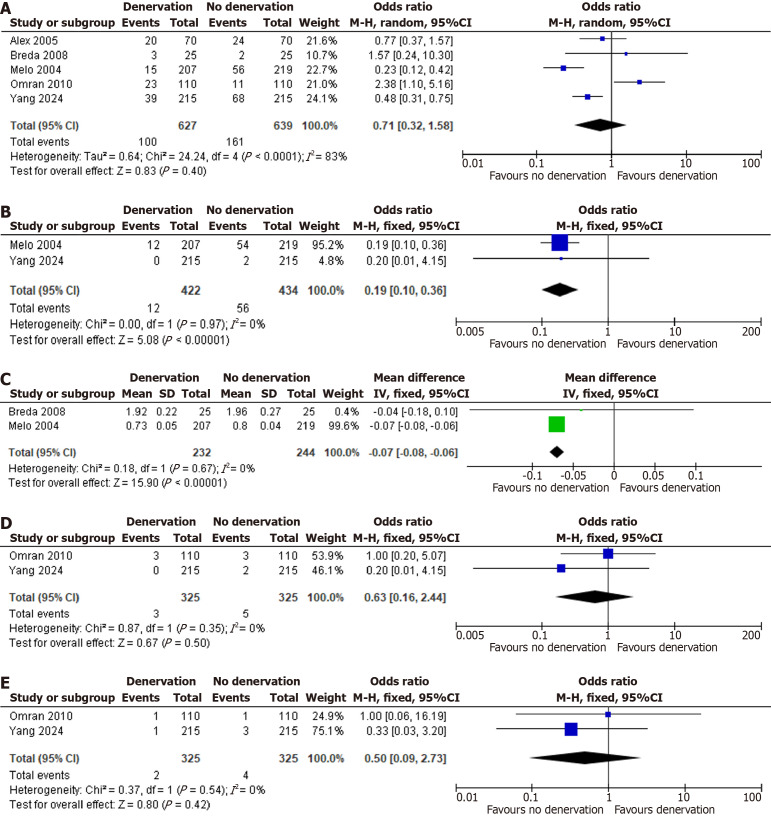
Results: Five studies (N = 1266) were included, with 627 patients undergoing cardiac denervation and 639 serving as controls. Denervation did not significantly reduce overall POAF [odds ratio = 0.71; 95% confidence interval (CI): 0.32-1.58; P = 0.40; I2 = 83%], but was associated with a significant reduction in persistent atrial fibrillation (odds ratio = 0.19; 95%CI: 0.10-0.36; P < 0.00001; I2 = 0%). Among secondary outcomes, only postoperative serum magnesium levels significantly reduced the denervation group (mean difference: -0.07 mmol/L; 95%CI: -0.08 to -0.06; P < 0.00001). Other outcomes, such as reoperation for bleeding, stroke/transient ischemic attack, length of hospital stay, 30-day mortality, and postoperative drainage, did not show any significant difference.
Conclusion: Surgical cardiac denervation does not significantly reduce overall POAF but does lower the incidence of persistent atrial fibrillation. It is also shown to decrease serum magnesium levels. Other outcomes, such as stroke, reoperation, and hospital stay, showed no significant differences.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


