{"title":"一项荟萃分析和系统综述,比较机器人和传统(腹腔镜或开放式)肝切除术在肝细胞癌患者围手术期的预后。","authors":"Lingbo Hu, Xingpeng Shi, Aidong Wang, Fabiao Zhang","doi":"10.1186/s12957-025-03983-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatectomy can be performed via laparoscopic liver resection (LLR), open liver resection (OLR), and robotic liver resection (RLR). However, the advantages of RLR over LLR and OLR with respect to the prognosis and perioperative outcomes of individuals with hepatocellular carcinoma (HCC) remain unclear. This study was designed to compare the perioperative and prognostic outcomes of RLR with those of LLR and OLR in patients with HCC.</p><p><strong>Methods: </strong>A comprehensive literature search was conducted in Embase, the Cochrane Library, PubMed, and Web of Science using the following keywords: \"liver resection,\" \"robotic,\" and \"hepatocellular carcinoma.\" The primary endpoints were overall survival (OS) and recurrence-free survival (RFS), with outcomes expressed as hazard ratios (HRs) and corresponding 95% confidence intervals (CIs). Secondary endpoints were perioperative outcomes, including resection margin status, intraoperative blood loss, transfusion requirement, operative time, conversion rate, postoperative complications, and length of hospital stay, reported as risk ratios (RRs) or mean differences (MDs) with 95% CIs.</p><p><strong>Results: </strong>Eighteen studies involving 4,098 patients were included. Twelve studies reported the long-term prognosis of patients, with six comparing RLR with LLR, four comparing RLR with OLR, and two comparing RLR with LLR and OLR. Sixteen studies reported perioperative outcomes. The meta-analysis illustrated that RLR was associated with improved RFS (HR 0.78, 95% CI 0.64-0.94; p = 0.0092) and OS (HR 0.72, 95% CI 0.56-0.92; p = 0.0101) compared with LLR. No significant differences in OS and RFS were observed between RLR and OLR. Compared with LLR, RLR was associated with a lower conversion rate to laparotomy (RR 0.50, 95% CI 0.31-0.79; p = 0.0034) and a longer operative time (MD 30.69 min, 95% CI 9.56-51.82; p = 0.0044). RLR also resulted in significantly lower rates of overall complications (RR 0.60, 95% CI 0.37-0.98; p = 0.0402), severe complications (RR 0.41, 95% CI 0.24-0.70; p = 0.0011, respectively), and a shorter hospital stay (MD - 3.70 days, 95% CI - 4.80 to - 2.61; p < 0.0001).</p><p><strong>Conclusion: </strong>In patients with HCC, RLR is associated with superior prognosis and perioperative outcomes compared with LLR and RLR exhibits better perioperative outcomes than OLR.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"23 1","pages":"348"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12481867/pdf/","citationCount":"0","resultStr":"{\"title\":\"A meta-analytic and systematic review to compare perioperative outcomes and prognosis between robotic and conventional (laparoscopic or open) liver resection in hepatocellular carcinoma cases.\",\"authors\":\"Lingbo Hu, Xingpeng Shi, Aidong Wang, Fabiao Zhang\",\"doi\":\"10.1186/s12957-025-03983-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hepatectomy can be performed via laparoscopic liver resection (LLR), open liver resection (OLR), and robotic liver resection (RLR). However, the advantages of RLR over LLR and OLR with respect to the prognosis and perioperative outcomes of individuals with hepatocellular carcinoma (HCC) remain unclear. This study was designed to compare the perioperative and prognostic outcomes of RLR with those of LLR and OLR in patients with HCC.</p><p><strong>Methods: </strong>A comprehensive literature search was conducted in Embase, the Cochrane Library, PubMed, and Web of Science using the following keywords: \\\"liver resection,\\\" \\\"robotic,\\\" and \\\"hepatocellular carcinoma.\\\" The primary endpoints were overall survival (OS) and recurrence-free survival (RFS), with outcomes expressed as hazard ratios (HRs) and corresponding 95% confidence intervals (CIs). Secondary endpoints were perioperative outcomes, including resection margin status, intraoperative blood loss, transfusion requirement, operative time, conversion rate, postoperative complications, and length of hospital stay, reported as risk ratios (RRs) or mean differences (MDs) with 95% CIs.</p><p><strong>Results: </strong>Eighteen studies involving 4,098 patients were included. Twelve studies reported the long-term prognosis of patients, with six comparing RLR with LLR, four comparing RLR with OLR, and two comparing RLR with LLR and OLR. Sixteen studies reported perioperative outcomes. The meta-analysis illustrated that RLR was associated with improved RFS (HR 0.78, 95% CI 0.64-0.94; p = 0.0092) and OS (HR 0.72, 95% CI 0.56-0.92; p = 0.0101) compared with LLR. No significant differences in OS and RFS were observed between RLR and OLR. Compared with LLR, RLR was associated with a lower conversion rate to laparotomy (RR 0.50, 95% CI 0.31-0.79; p = 0.0034) and a longer operative time (MD 30.69 min, 95% CI 9.56-51.82; p = 0.0044). RLR also resulted in significantly lower rates of overall complications (RR 0.60, 95% CI 0.37-0.98; p = 0.0402), severe complications (RR 0.41, 95% CI 0.24-0.70; p = 0.0011, respectively), and a shorter hospital stay (MD - 3.70 days, 95% CI - 4.80 to - 2.61; p < 0.0001).</p><p><strong>Conclusion: </strong>In patients with HCC, RLR is associated with superior prognosis and perioperative outcomes compared with LLR and RLR exhibits better perioperative outcomes than OLR.</p>\",\"PeriodicalId\":23856,\"journal\":{\"name\":\"World Journal of Surgical Oncology\",\"volume\":\"23 1\",\"pages\":\"348\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12481867/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Surgical Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12957-025-03983-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-025-03983-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
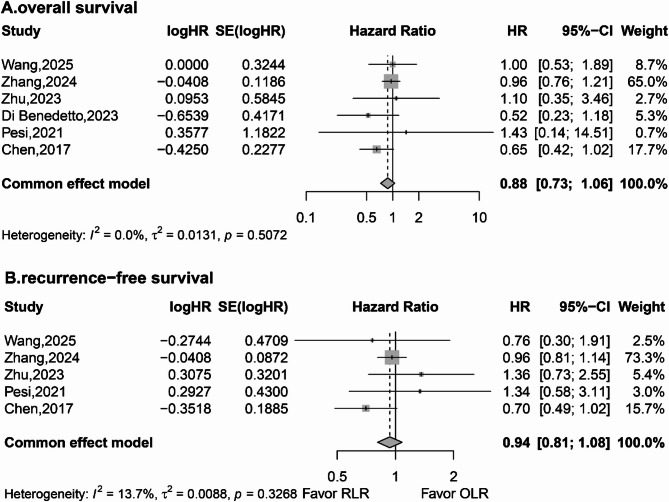
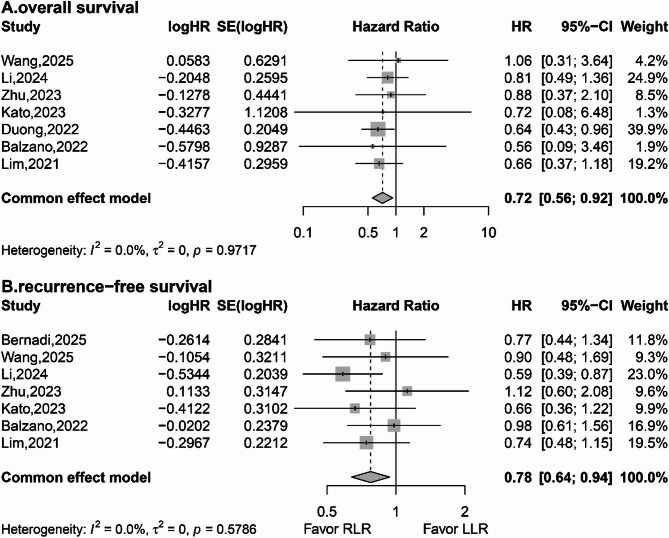
背景:肝切除术可通过腹腔镜肝切除术(LLR)、开放式肝切除术(OLR)和机器人肝切除术(RLR)进行。然而,在肝细胞癌(HCC)患者的预后和围手术期结局方面,RLR相对于LLR和OLR的优势尚不清楚。本研究旨在比较HCC患者RLR与LLR和OLR的围手术期和预后。方法:在Embase、Cochrane图书馆、PubMed和Web of Science中进行全面的文献检索,检索关键词为“肝切除”、“机器人”和“肝细胞癌”。主要终点是总生存期(OS)和无复发生存期(RFS),结果用风险比(hr)和相应的95%置信区间(ci)表示。次要终点是围手术期结局,包括切除边缘状况、术中出血量、输血需求、手术时间、转化率、术后并发症和住院时间,报告为95% ci的风险比(rr)或平均差异(MDs)。结果:纳入18项研究,涉及4098例患者。12项研究报道了患者的长期预后,其中6项比较RLR与LLR, 4项比较RLR与OLR, 2项比较RLR与LLR和OLR。16项研究报告了围手术期结果。meta分析显示,与LLR相比,RLR与改善的RFS (HR 0.78, 95% CI 0.64-0.94; p = 0.0092)和OS (HR 0.72, 95% CI 0.56-0.92; p = 0.0101)相关。RLR组和OLR组的OS和RFS无显著差异。与LLR相比,RLR与较低的开腹转复率(RR 0.50, 95% CI 0.31-0.79; p = 0.0034)和较长的手术时间(MD 30.69 min, 95% CI 9.56-51.82; p = 0.0044)相关。RLR的总并发症发生率(RR 0.60, 95% CI 0.37-0.98; p = 0.0402)、严重并发症发生率(RR 0.41, 95% CI 0.24-0.70; p = 0.0011)、住院时间(MD - 3.70天,95% CI - 4.80 ~ - 2.61; p)也显著降低。结论:HCC患者RLR的预后和围手术期结局优于LLR, RLR的围手术期结局优于OLR。
A meta-analytic and systematic review to compare perioperative outcomes and prognosis between robotic and conventional (laparoscopic or open) liver resection in hepatocellular carcinoma cases.
Background: Hepatectomy can be performed via laparoscopic liver resection (LLR), open liver resection (OLR), and robotic liver resection (RLR). However, the advantages of RLR over LLR and OLR with respect to the prognosis and perioperative outcomes of individuals with hepatocellular carcinoma (HCC) remain unclear. This study was designed to compare the perioperative and prognostic outcomes of RLR with those of LLR and OLR in patients with HCC.
Methods: A comprehensive literature search was conducted in Embase, the Cochrane Library, PubMed, and Web of Science using the following keywords: "liver resection," "robotic," and "hepatocellular carcinoma." The primary endpoints were overall survival (OS) and recurrence-free survival (RFS), with outcomes expressed as hazard ratios (HRs) and corresponding 95% confidence intervals (CIs). Secondary endpoints were perioperative outcomes, including resection margin status, intraoperative blood loss, transfusion requirement, operative time, conversion rate, postoperative complications, and length of hospital stay, reported as risk ratios (RRs) or mean differences (MDs) with 95% CIs.
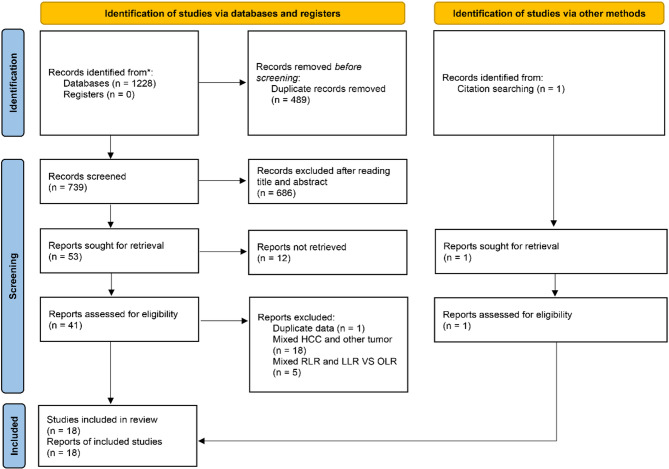
Results: Eighteen studies involving 4,098 patients were included. Twelve studies reported the long-term prognosis of patients, with six comparing RLR with LLR, four comparing RLR with OLR, and two comparing RLR with LLR and OLR. Sixteen studies reported perioperative outcomes. The meta-analysis illustrated that RLR was associated with improved RFS (HR 0.78, 95% CI 0.64-0.94; p = 0.0092) and OS (HR 0.72, 95% CI 0.56-0.92; p = 0.0101) compared with LLR. No significant differences in OS and RFS were observed between RLR and OLR. Compared with LLR, RLR was associated with a lower conversion rate to laparotomy (RR 0.50, 95% CI 0.31-0.79; p = 0.0034) and a longer operative time (MD 30.69 min, 95% CI 9.56-51.82; p = 0.0044). RLR also resulted in significantly lower rates of overall complications (RR 0.60, 95% CI 0.37-0.98; p = 0.0402), severe complications (RR 0.41, 95% CI 0.24-0.70; p = 0.0011, respectively), and a shorter hospital stay (MD - 3.70 days, 95% CI - 4.80 to - 2.61; p < 0.0001).
Conclusion: In patients with HCC, RLR is associated with superior prognosis and perioperative outcomes compared with LLR and RLR exhibits better perioperative outcomes than OLR.
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


