{"title":"切除胰腺导管腺癌早期复发的术前风险分层:细胞外体积的新型平衡相计算机断层扫描生物标志物。","authors":"Zhi-Wei Zhang, Hao-Tian Liu, Zhuo-Hang Zhou, Hong-Fan Liao, Lan-Ling Zhang, Yong-Mei Li, Hong-Wei Liang","doi":"10.3748/wjg.v31.i35.109687","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Predicting early recurrence (ER), (≤ 12 months) after pancreatic ductal adenocarcinoma (PDAC) resection remains challenging. Preoperative biomarkers such as carbohydrate antigen 19-9 (CA19-9) and computed tomography (CT) lack optimal specificity and reproducibility. Extracellular volume (ECV), measured on equilibrium-phase CT to quantify stromal fibrosis, correlates with PDAC progression but its utility for ER prediction is unknown. This study evaluates preoperative CT-ECV as a novel biomarker to predict ER following curative-intent PDAC resection.</p><p><strong>Aim: </strong>To investigate the utility of CT-ECV for preoperative prediction of ER in PDAC patients after R0 resection.</p><p><strong>Methods: </strong>This retrospective study included 93 PDAC patients undergoing R0 resection and preoperative pancreatic CT from January 2020 to November 2023. Clinical and CT features were analyzed. ECV was calculated using unenhanced and equilibrium-phase CT. Univariable and multivariable Cox regression identified ER predictors, followed by receiver operating characteristic analysis. Recurrence-free survival (RFS) was assessed by the Kaplan-Meier method.</p><p><strong>Results: </strong>Multivariable analysis identified elevated CT-ECV [hazard ratio (HR) = 1.05; 95% confidence interval (CI): 1.02-1.09; <i>P</i> = 0.003], high preoperative CA19-9 (HR = 1.00; 95%CI: 1.00-1.00; <i>P</i> = 0.002), and poor tumor grade (HR = 2.51; 95%CI: 1.20-5.22; <i>P</i> = 0.014) as independent ER predictors. CT-ECV demonstrated comparable predictive accuracy to tumor grade [areas under the curve (AUC): 0.736 <i>vs</i> 0.650; <i>P</i> = 0.202]. Combining CT-ECV and CA19-9 achieved a higher AUC than tumor grade alone (0.759 <i>vs</i> 0.650; <i>P</i> < 0.05). Kaplan-Meier analysis revealed significantly shorter RFS in patients with low CT-ECV (≤ 35.37%), elevated CA19-9 (> 55 U/mL), or poorly differentiated tumors compared to those with high CT-ECV (> 35.37%), low CA19-9 (≤ 55 U/mL), or moderately/well-differentiated tumors.</p><p><strong>Conclusion: </strong>CT-derived ECV is a promising non-invasive biomarker for preoperative ER prediction in PDAC. Combined with CA19-9, it outperforms tumor grade in stratifying recurrence risk, offering a clinically actionable tool for optimizing postoperative management.</p>","PeriodicalId":23778,"journal":{"name":"World Journal of Gastroenterology","volume":"31 35","pages":"109687"},"PeriodicalIF":5.4000,"publicationDate":"2025-09-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476667/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative risk stratification of early recurrence in resected pancreatic ductal adenocarcinoma: Novel equilibrium-phase-computed tomography biomarker of extracellular volume.\",\"authors\":\"Zhi-Wei Zhang, Hao-Tian Liu, Zhuo-Hang Zhou, Hong-Fan Liao, Lan-Ling Zhang, Yong-Mei Li, Hong-Wei Liang\",\"doi\":\"10.3748/wjg.v31.i35.109687\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Predicting early recurrence (ER), (≤ 12 months) after pancreatic ductal adenocarcinoma (PDAC) resection remains challenging. Preoperative biomarkers such as carbohydrate antigen 19-9 (CA19-9) and computed tomography (CT) lack optimal specificity and reproducibility. Extracellular volume (ECV), measured on equilibrium-phase CT to quantify stromal fibrosis, correlates with PDAC progression but its utility for ER prediction is unknown. This study evaluates preoperative CT-ECV as a novel biomarker to predict ER following curative-intent PDAC resection.</p><p><strong>Aim: </strong>To investigate the utility of CT-ECV for preoperative prediction of ER in PDAC patients after R0 resection.</p><p><strong>Methods: </strong>This retrospective study included 93 PDAC patients undergoing R0 resection and preoperative pancreatic CT from January 2020 to November 2023. Clinical and CT features were analyzed. ECV was calculated using unenhanced and equilibrium-phase CT. Univariable and multivariable Cox regression identified ER predictors, followed by receiver operating characteristic analysis. Recurrence-free survival (RFS) was assessed by the Kaplan-Meier method.</p><p><strong>Results: </strong>Multivariable analysis identified elevated CT-ECV [hazard ratio (HR) = 1.05; 95% confidence interval (CI): 1.02-1.09; <i>P</i> = 0.003], high preoperative CA19-9 (HR = 1.00; 95%CI: 1.00-1.00; <i>P</i> = 0.002), and poor tumor grade (HR = 2.51; 95%CI: 1.20-5.22; <i>P</i> = 0.014) as independent ER predictors. CT-ECV demonstrated comparable predictive accuracy to tumor grade [areas under the curve (AUC): 0.736 <i>vs</i> 0.650; <i>P</i> = 0.202]. Combining CT-ECV and CA19-9 achieved a higher AUC than tumor grade alone (0.759 <i>vs</i> 0.650; <i>P</i> < 0.05). Kaplan-Meier analysis revealed significantly shorter RFS in patients with low CT-ECV (≤ 35.37%), elevated CA19-9 (> 55 U/mL), or poorly differentiated tumors compared to those with high CT-ECV (> 35.37%), low CA19-9 (≤ 55 U/mL), or moderately/well-differentiated tumors.</p><p><strong>Conclusion: </strong>CT-derived ECV is a promising non-invasive biomarker for preoperative ER prediction in PDAC. Combined with CA19-9, it outperforms tumor grade in stratifying recurrence risk, offering a clinically actionable tool for optimizing postoperative management.</p>\",\"PeriodicalId\":23778,\"journal\":{\"name\":\"World Journal of Gastroenterology\",\"volume\":\"31 35\",\"pages\":\"109687\"},\"PeriodicalIF\":5.4000,\"publicationDate\":\"2025-09-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476667/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3748/wjg.v31.i35.109687\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3748/wjg.v31.i35.109687","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:预测胰导管腺癌(PDAC)切除术后早期复发(≤12个月)仍然具有挑战性。术前生物标志物如碳水化合物抗原19-9 (CA19-9)和计算机断层扫描(CT)缺乏最佳的特异性和可重复性。细胞外体积(ECV),通过平衡期CT测量来量化间质纤维化,与PDAC进展相关,但其用于ER预测的效用尚不清楚。这项研究评估了术前CT-ECV作为一种新的生物标志物来预测治疗意图的PDAC切除术后的ER。目的:探讨CT-ECV在PDAC患者R0切除术后ER术前预测中的应用价值。方法:本回顾性研究包括93例PDAC患者,于2020年1月至2023年11月行R0切除术和术前胰腺CT。分析临床及CT表现。采用非增强和平衡相CT计算ECV。单变量和多变量Cox回归确定了ER预测因子,然后进行了受试者工作特征分析。采用Kaplan-Meier法评估无复发生存期(RFS)。结果:多变量分析发现CT-ECV升高[危险比(HR) = 1.05;95%置信区间(CI): 1.02-1.09;P = 0.003],术前高CA19-9 (HR = 1.00; 95%CI: 1.00-1.00; P = 0.002)和肿瘤分级差(HR = 2.51; 95%CI: 1.20-5.22; P = 0.014)是ER的独立预测因子。CT-ECV对肿瘤分级的预测准确度相当[曲线下面积(AUC): 0.736 vs 0.650;P = 0.202]。CT-ECV联合CA19-9的AUC高于单纯肿瘤分级(0.759 vs 0.650, P < 0.05)。Kaplan-Meier分析显示,与高CT-ECV(> 35.37%)、低CA19-9(≤55 U/mL)或中/高分化肿瘤患者相比,低CT-ECV(≤35.37%)、低CA19-9(≤55 U/mL)或低分化肿瘤患者的RFS显著缩短。结论:ct衍生的ECV是一种很有希望用于PDAC术前ER预测的无创生物标志物。与CA19-9联合使用,在复发风险分层方面优于肿瘤分级,为优化术后管理提供了临床可操作的工具。
Preoperative risk stratification of early recurrence in resected pancreatic ductal adenocarcinoma: Novel equilibrium-phase-computed tomography biomarker of extracellular volume.
Background: Predicting early recurrence (ER), (≤ 12 months) after pancreatic ductal adenocarcinoma (PDAC) resection remains challenging. Preoperative biomarkers such as carbohydrate antigen 19-9 (CA19-9) and computed tomography (CT) lack optimal specificity and reproducibility. Extracellular volume (ECV), measured on equilibrium-phase CT to quantify stromal fibrosis, correlates with PDAC progression but its utility for ER prediction is unknown. This study evaluates preoperative CT-ECV as a novel biomarker to predict ER following curative-intent PDAC resection.
Aim: To investigate the utility of CT-ECV for preoperative prediction of ER in PDAC patients after R0 resection.
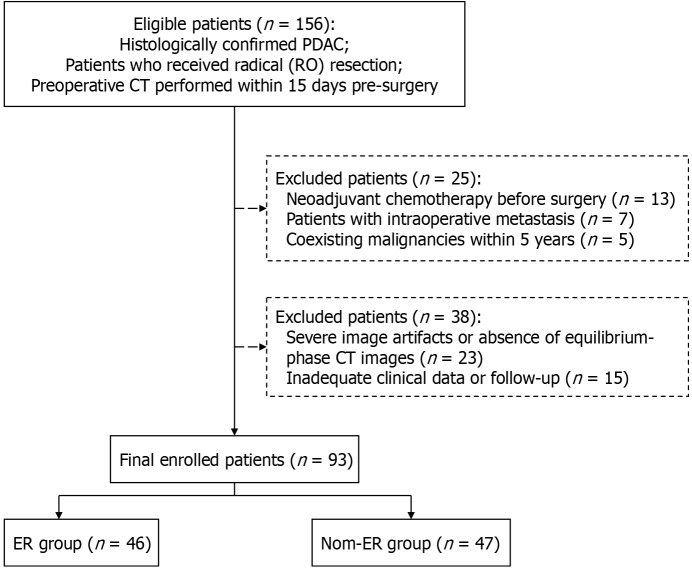
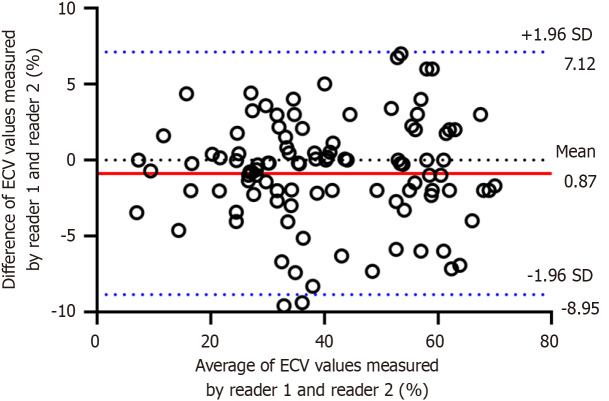
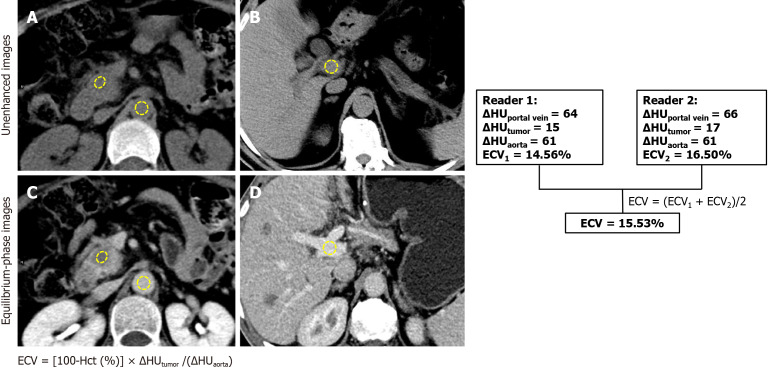
Methods: This retrospective study included 93 PDAC patients undergoing R0 resection and preoperative pancreatic CT from January 2020 to November 2023. Clinical and CT features were analyzed. ECV was calculated using unenhanced and equilibrium-phase CT. Univariable and multivariable Cox regression identified ER predictors, followed by receiver operating characteristic analysis. Recurrence-free survival (RFS) was assessed by the Kaplan-Meier method.
Results: Multivariable analysis identified elevated CT-ECV [hazard ratio (HR) = 1.05; 95% confidence interval (CI): 1.02-1.09; P = 0.003], high preoperative CA19-9 (HR = 1.00; 95%CI: 1.00-1.00; P = 0.002), and poor tumor grade (HR = 2.51; 95%CI: 1.20-5.22; P = 0.014) as independent ER predictors. CT-ECV demonstrated comparable predictive accuracy to tumor grade [areas under the curve (AUC): 0.736 vs 0.650; P = 0.202]. Combining CT-ECV and CA19-9 achieved a higher AUC than tumor grade alone (0.759 vs 0.650; P < 0.05). Kaplan-Meier analysis revealed significantly shorter RFS in patients with low CT-ECV (≤ 35.37%), elevated CA19-9 (> 55 U/mL), or poorly differentiated tumors compared to those with high CT-ECV (> 35.37%), low CA19-9 (≤ 55 U/mL), or moderately/well-differentiated tumors.
Conclusion: CT-derived ECV is a promising non-invasive biomarker for preoperative ER prediction in PDAC. Combined with CA19-9, it outperforms tumor grade in stratifying recurrence risk, offering a clinically actionable tool for optimizing postoperative management.
期刊介绍:
The primary aims of the WJG are to improve diagnostic, therapeutic and preventive modalities and the skills of clinicians and to guide clinical practice in gastroenterology and hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


