{"title":"早期结直肠癌及癌前病变内镜下粘膜下剥离术后迟发性出血的风险建模。","authors":"Jun Qian, Ya-Li Tao, Shu-Sen Zheng","doi":"10.4240/wjgs.v17.i9.107326","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As a minimally invasive technique, endoscopic submucosal dissection (ESD) is widely used in treating early colorectal cancer (ECRC) and precancerous lesions (PCLs). However, a common postoperative complication - delayed postoperative bleeding (DPOB) - can significantly hinder patient recovery.</p><p><strong>Aim: </strong>To build and validate a predictive model for assessing post-ESD DPOB risk in ECRC and PCL patients, utilizing logistic regression methodology.</p><p><strong>Methods: </strong>A retrospective review was conducted on ECRC/PCL 302 patients who received ESD at our hospital between July 2021 and July 2024. The cohort was stratified based on the incidence of DPOB following ESD, forming DPOB and non-DPOB groups. Through allocation, they were further allocated into model and validation cohorts. Clinical variables from both cohorts were collated and subjected to univariate analysis to determine potential factors associated with post-ESD DPOB. Subsequently, we constructed a predictive model for DPOB risk employing logistic regression analysis. Model performance assessment used receiver operating characteristic curves in both the training and validation cohorts, with internal validation accomplished <i>via</i> 10-fold cross-validation.</p><p><strong>Results: </strong>The occurrence rate of DPOB was 9.93%. Univariate analysis revealed that the number of lesions, lesion size, lesion location, degree of submucosal fibrosis, and intraoperative bleeding were significantly associated with DPOB. Binary logistic regression analysis identified the number of lesions, lesion size, lesion location, and degree of submucosal fibrosis as independent DPOB determinants. A nomogram that was developed to quantify the DPOB risk exhibited that an increment in the total score corresponded to an increased risk. The model achieved area under the curve values of 0.831 and 0.821 in the model and validation groups, respectively, with <i>P</i> values of 0.853 and 0.203 in the Hosmer-Lemeshow test. The model demonstrated robust discriminative performance, with an average area under the curve of 0.795 (95% confidence interval: 0.702-0.887) in 10-fold cross-validation.</p><p><strong>Conclusion: </strong>Collectively, the presence of multiple lesions, lesion size of ≥ 3 cm, lesion localization in the rectum, and severe fibrosis are significant independent predictors of DPOB in patients undergoing surgery for ECRC or PCLs. The proposed risk prediction model, which integrates these factors, demonstrates excellent predictive accuracy and clinical utility, thereby providing a valuable tool for risk stratification and postoperative management in this patient population.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"17 9","pages":"107326"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476782/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk modeling of delayed postoperative bleeding after endoscopic submucosal dissection for early colorectal cancer and precancerous lesions.\",\"authors\":\"Jun Qian, Ya-Li Tao, Shu-Sen Zheng\",\"doi\":\"10.4240/wjgs.v17.i9.107326\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>As a minimally invasive technique, endoscopic submucosal dissection (ESD) is widely used in treating early colorectal cancer (ECRC) and precancerous lesions (PCLs). However, a common postoperative complication - delayed postoperative bleeding (DPOB) - can significantly hinder patient recovery.</p><p><strong>Aim: </strong>To build and validate a predictive model for assessing post-ESD DPOB risk in ECRC and PCL patients, utilizing logistic regression methodology.</p><p><strong>Methods: </strong>A retrospective review was conducted on ECRC/PCL 302 patients who received ESD at our hospital between July 2021 and July 2024. The cohort was stratified based on the incidence of DPOB following ESD, forming DPOB and non-DPOB groups. Through allocation, they were further allocated into model and validation cohorts. Clinical variables from both cohorts were collated and subjected to univariate analysis to determine potential factors associated with post-ESD DPOB. Subsequently, we constructed a predictive model for DPOB risk employing logistic regression analysis. Model performance assessment used receiver operating characteristic curves in both the training and validation cohorts, with internal validation accomplished <i>via</i> 10-fold cross-validation.</p><p><strong>Results: </strong>The occurrence rate of DPOB was 9.93%. Univariate analysis revealed that the number of lesions, lesion size, lesion location, degree of submucosal fibrosis, and intraoperative bleeding were significantly associated with DPOB. Binary logistic regression analysis identified the number of lesions, lesion size, lesion location, and degree of submucosal fibrosis as independent DPOB determinants. A nomogram that was developed to quantify the DPOB risk exhibited that an increment in the total score corresponded to an increased risk. The model achieved area under the curve values of 0.831 and 0.821 in the model and validation groups, respectively, with <i>P</i> values of 0.853 and 0.203 in the Hosmer-Lemeshow test. The model demonstrated robust discriminative performance, with an average area under the curve of 0.795 (95% confidence interval: 0.702-0.887) in 10-fold cross-validation.</p><p><strong>Conclusion: </strong>Collectively, the presence of multiple lesions, lesion size of ≥ 3 cm, lesion localization in the rectum, and severe fibrosis are significant independent predictors of DPOB in patients undergoing surgery for ECRC or PCLs. The proposed risk prediction model, which integrates these factors, demonstrates excellent predictive accuracy and clinical utility, thereby providing a valuable tool for risk stratification and postoperative management in this patient population.</p>\",\"PeriodicalId\":23759,\"journal\":{\"name\":\"World Journal of Gastrointestinal Surgery\",\"volume\":\"17 9\",\"pages\":\"107326\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-09-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476782/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4240/wjgs.v17.i9.107326\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v17.i9.107326","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Risk modeling of delayed postoperative bleeding after endoscopic submucosal dissection for early colorectal cancer and precancerous lesions.
Background: As a minimally invasive technique, endoscopic submucosal dissection (ESD) is widely used in treating early colorectal cancer (ECRC) and precancerous lesions (PCLs). However, a common postoperative complication - delayed postoperative bleeding (DPOB) - can significantly hinder patient recovery.
Aim: To build and validate a predictive model for assessing post-ESD DPOB risk in ECRC and PCL patients, utilizing logistic regression methodology.
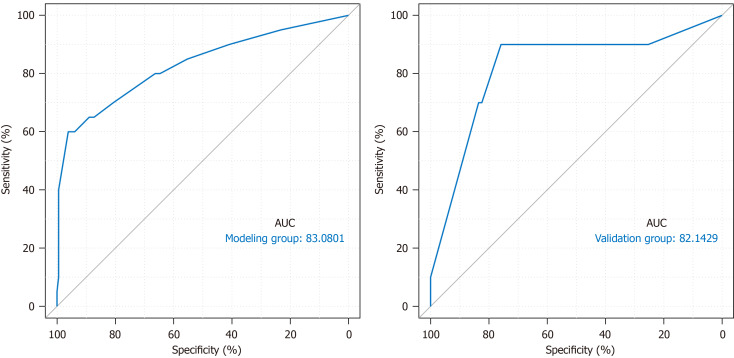
Methods: A retrospective review was conducted on ECRC/PCL 302 patients who received ESD at our hospital between July 2021 and July 2024. The cohort was stratified based on the incidence of DPOB following ESD, forming DPOB and non-DPOB groups. Through allocation, they were further allocated into model and validation cohorts. Clinical variables from both cohorts were collated and subjected to univariate analysis to determine potential factors associated with post-ESD DPOB. Subsequently, we constructed a predictive model for DPOB risk employing logistic regression analysis. Model performance assessment used receiver operating characteristic curves in both the training and validation cohorts, with internal validation accomplished via 10-fold cross-validation.
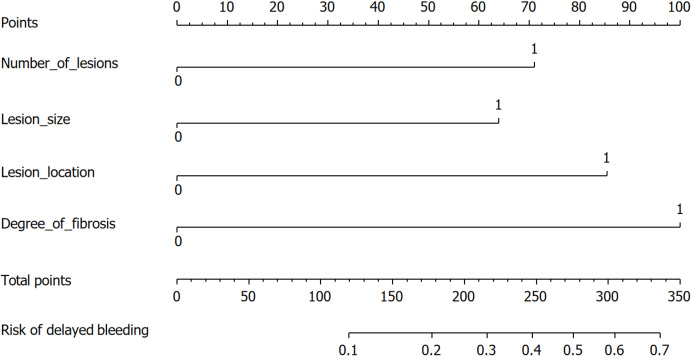
Results: The occurrence rate of DPOB was 9.93%. Univariate analysis revealed that the number of lesions, lesion size, lesion location, degree of submucosal fibrosis, and intraoperative bleeding were significantly associated with DPOB. Binary logistic regression analysis identified the number of lesions, lesion size, lesion location, and degree of submucosal fibrosis as independent DPOB determinants. A nomogram that was developed to quantify the DPOB risk exhibited that an increment in the total score corresponded to an increased risk. The model achieved area under the curve values of 0.831 and 0.821 in the model and validation groups, respectively, with P values of 0.853 and 0.203 in the Hosmer-Lemeshow test. The model demonstrated robust discriminative performance, with an average area under the curve of 0.795 (95% confidence interval: 0.702-0.887) in 10-fold cross-validation.
Conclusion: Collectively, the presence of multiple lesions, lesion size of ≥ 3 cm, lesion localization in the rectum, and severe fibrosis are significant independent predictors of DPOB in patients undergoing surgery for ECRC or PCLs. The proposed risk prediction model, which integrates these factors, demonstrates excellent predictive accuracy and clinical utility, thereby providing a valuable tool for risk stratification and postoperative management in this patient population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


