{"title":"胃近端肿瘤双道重建:临床和功能结果的系统回顾。","authors":"Enver Ilhan, Gökalp Okut","doi":"10.4240/wjgs.v17.i9.109030","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Proximal gastrectomy (PG) with double tract reconstruction (DTR) has recently emerged as a function-preserving alternative to total gastrectomy (TG) with Roux-en-Y (RNY) reconstruction in patients with proximally located gastric cancer.</p><p><strong>Aim: </strong>To evaluate the current evidence comparing PG-DTR with TG-RNY in terms of perioperative outcomes, long-term survival, complication rates, nutritional status and reflux esophagitis.</p><p><strong>Methods: </strong>A systematic literature search was conducted using PubMed, MEDLINE, Web of Science and the Cochrane Library for studies published between 2010 and January 2025. Search terms included gastric cancer, DTR and TG. Trials comparing PG-DTR with TG-RNY or PG-esophagogastrostomy (EG) were included. Data on operative details, lymph node yield, complications (Clavien-Dindo ≥ III), nutritional markers and incidence of reflux were extracted. Nineteen trials met the inclusion criteria. The review followed the PRISMA guidelines.</p><p><strong>Results: </strong>PG-DTR was found to have comparable long-term oncological outcomes to TG-RNY, despite a lower extent of lymph node dissection. Operative time and intraoperative blood loss were generally similar, with some studies favouring PG-DTR. Rates of major postoperative complications were comparable between techniques. Notably, PG-DTR showed a significantly lower incidence of reflux esophagitis than PG-EG and was comparable or superior to TG-RNY in reflux control. Nutritionally, PG-DTR was associated with better post-operative weight maintenance and biochemical parameters such as haemoglobin, albumin and vitamin B12 levels compared to TG-RNY. No significant nutritional differences were observed between PG-DTR and PG-EG. PG-DTR appears to offer a balanced approach to the surgical treatment of proximal gastric cancer, combining oncological safety with functional and nutritional benefits.</p><p><strong>Conclusion: </strong>Its superiority over TG-RNY in postoperative nutrition and reflux prevention, together with comparable complication rates and survival, supports its consideration as a preferred reconstruction method in selected patients.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"17 9","pages":"109030"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476753/pdf/","citationCount":"0","resultStr":"{\"title\":\"Double tract reconstruction in proximal gastric tumors: A systematic review of clinical and functional outcomes.\",\"authors\":\"Enver Ilhan, Gökalp Okut\",\"doi\":\"10.4240/wjgs.v17.i9.109030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Proximal gastrectomy (PG) with double tract reconstruction (DTR) has recently emerged as a function-preserving alternative to total gastrectomy (TG) with Roux-en-Y (RNY) reconstruction in patients with proximally located gastric cancer.</p><p><strong>Aim: </strong>To evaluate the current evidence comparing PG-DTR with TG-RNY in terms of perioperative outcomes, long-term survival, complication rates, nutritional status and reflux esophagitis.</p><p><strong>Methods: </strong>A systematic literature search was conducted using PubMed, MEDLINE, Web of Science and the Cochrane Library for studies published between 2010 and January 2025. Search terms included gastric cancer, DTR and TG. Trials comparing PG-DTR with TG-RNY or PG-esophagogastrostomy (EG) were included. Data on operative details, lymph node yield, complications (Clavien-Dindo ≥ III), nutritional markers and incidence of reflux were extracted. Nineteen trials met the inclusion criteria. The review followed the PRISMA guidelines.</p><p><strong>Results: </strong>PG-DTR was found to have comparable long-term oncological outcomes to TG-RNY, despite a lower extent of lymph node dissection. Operative time and intraoperative blood loss were generally similar, with some studies favouring PG-DTR. Rates of major postoperative complications were comparable between techniques. Notably, PG-DTR showed a significantly lower incidence of reflux esophagitis than PG-EG and was comparable or superior to TG-RNY in reflux control. Nutritionally, PG-DTR was associated with better post-operative weight maintenance and biochemical parameters such as haemoglobin, albumin and vitamin B12 levels compared to TG-RNY. No significant nutritional differences were observed between PG-DTR and PG-EG. PG-DTR appears to offer a balanced approach to the surgical treatment of proximal gastric cancer, combining oncological safety with functional and nutritional benefits.</p><p><strong>Conclusion: </strong>Its superiority over TG-RNY in postoperative nutrition and reflux prevention, together with comparable complication rates and survival, supports its consideration as a preferred reconstruction method in selected patients.</p>\",\"PeriodicalId\":23759,\"journal\":{\"name\":\"World Journal of Gastrointestinal Surgery\",\"volume\":\"17 9\",\"pages\":\"109030\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-09-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476753/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4240/wjgs.v17.i9.109030\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v17.i9.109030","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:近端胃切除术(PG)联合双胃道重建术(DTR)最近被认为是一种功能保留替代全胃切除术(TG)联合Roux-en-Y (RNY)重建术治疗近端胃癌的方法。目的:评价PG-DTR与TG-RNY在围手术期结局、长期生存、并发症发生率、营养状况和反流性食管炎方面的比较证据。方法:系统检索PubMed、MEDLINE、Web of Science和Cochrane图书馆2010年至2025年1月间发表的研究。搜索词包括胃癌、DTR和TG。包括将PG-DTR与TG-RNY或pg -食管胃造口术(EG)进行比较的试验。提取手术细节、淋巴结产量、并发症(Clavien-Dindo≥III)、营养指标和反流发生率的数据。19项试验符合纳入标准。审查遵循了PRISMA的指导方针。结果:PG-DTR与TG-RNY具有相当的长期肿瘤预后,尽管淋巴结清扫程度较低。手术时间和术中出血量大致相似,一些研究倾向于PG-DTR。两种技术的主要术后并发症发生率相当。值得注意的是,PG-DTR的反流性食管炎发生率明显低于PG-EG,在反流控制方面与TG-RNY相当或优于TG-RNY。在营养方面,与TG-RNY相比,PG-DTR与更好的术后体重维持和生化参数(如血红蛋白、白蛋白和维生素B12水平)相关。PG-DTR和PG-EG在营养方面没有显著差异。PG-DTR似乎为近端胃癌的手术治疗提供了一种平衡的方法,将肿瘤安全性与功能和营养益处相结合。结论:与TG-RNY相比,其在术后营养和反流预防方面的优势,以及相当的并发症发生率和生存率,支持将其作为特定患者的首选重建方法。
Double tract reconstruction in proximal gastric tumors: A systematic review of clinical and functional outcomes.
Background: Proximal gastrectomy (PG) with double tract reconstruction (DTR) has recently emerged as a function-preserving alternative to total gastrectomy (TG) with Roux-en-Y (RNY) reconstruction in patients with proximally located gastric cancer.
Aim: To evaluate the current evidence comparing PG-DTR with TG-RNY in terms of perioperative outcomes, long-term survival, complication rates, nutritional status and reflux esophagitis.
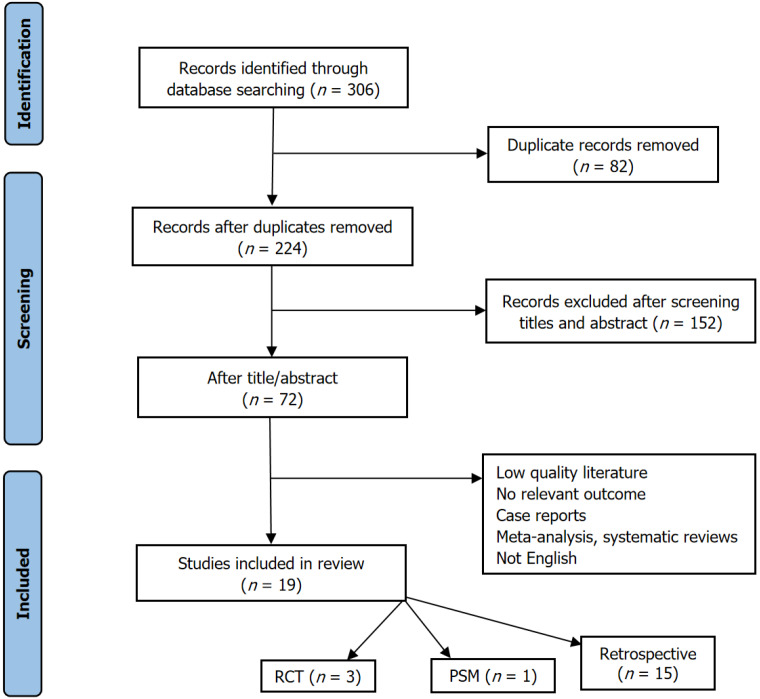
Methods: A systematic literature search was conducted using PubMed, MEDLINE, Web of Science and the Cochrane Library for studies published between 2010 and January 2025. Search terms included gastric cancer, DTR and TG. Trials comparing PG-DTR with TG-RNY or PG-esophagogastrostomy (EG) were included. Data on operative details, lymph node yield, complications (Clavien-Dindo ≥ III), nutritional markers and incidence of reflux were extracted. Nineteen trials met the inclusion criteria. The review followed the PRISMA guidelines.
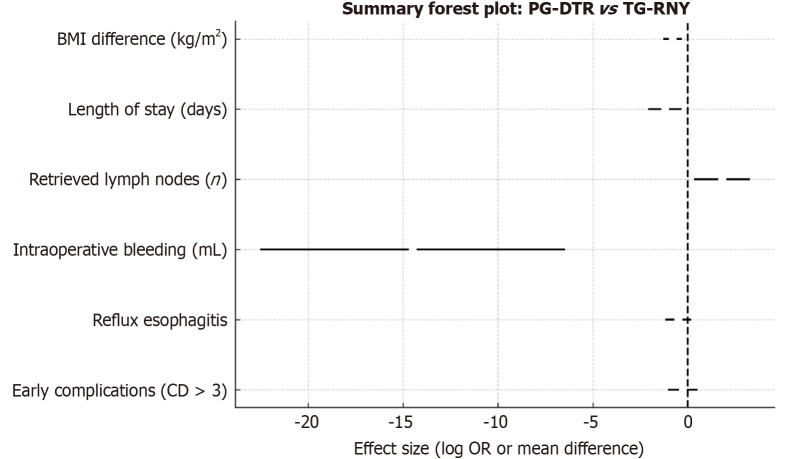
Results: PG-DTR was found to have comparable long-term oncological outcomes to TG-RNY, despite a lower extent of lymph node dissection. Operative time and intraoperative blood loss were generally similar, with some studies favouring PG-DTR. Rates of major postoperative complications were comparable between techniques. Notably, PG-DTR showed a significantly lower incidence of reflux esophagitis than PG-EG and was comparable or superior to TG-RNY in reflux control. Nutritionally, PG-DTR was associated with better post-operative weight maintenance and biochemical parameters such as haemoglobin, albumin and vitamin B12 levels compared to TG-RNY. No significant nutritional differences were observed between PG-DTR and PG-EG. PG-DTR appears to offer a balanced approach to the surgical treatment of proximal gastric cancer, combining oncological safety with functional and nutritional benefits.
Conclusion: Its superiority over TG-RNY in postoperative nutrition and reflux prevention, together with comparable complication rates and survival, supports its consideration as a preferred reconstruction method in selected patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


