Shunsuke Todani, Kazuhiro Shimizu, Shuji Sato, Kohji Shirai, Atsuhito Saiki
{"title":"透析患者心踝血管指数纵向变化与主动脉狭窄进展之间的关系:一项回顾性研究。","authors":"Shunsuke Todani, Kazuhiro Shimizu, Shuji Sato, Kohji Shirai, Atsuhito Saiki","doi":"10.7759/cureus.93263","DOIUrl":null,"url":null,"abstract":"<p><p>Objective In dialysis patients, echocardiography often underestimates the progression of aortic stenosis (AS) due to blood pressure fluctuations and extensive calcification that obscure standard indices. We evaluated whether serial changes in the cardio-ankle vascular index (CAVI), a blood pressure-independent marker of arterial stiffness, can anticipate severe AS and guide the timing of valve replacement. Methods This single-center, retrospective study screened 1,169 maintenance dialysis patients (2015-2023). Forty-one patients who underwent surgical or transcatheter aortic valve replacement (AVR/TAVR) had valid CAVI measurements at four time points: 2 years and 1 year before surgery, immediately before surgery, and 1 year after surgery. The -2-year time point served as the baseline. Hemodynamic, echocardiographic, and laboratory data were analyzed using the Friedman and Wilcoxon tests. Severe AS progression was defined as a new mean pressure gradient (meanPG) ≥ 40 mmHg. Determinants of progression were identified using multivariable logistic regression. Results Median CAVI declined from 10.2 to 9.4 over the two years preceding surgery (p < 0.001) and rose to 11.1 one year post-AVR/TAVR (p < 0.001). Simultaneously, ejection time increased, ejection fraction decreased, and Vmax, maxPG, stroke volume, and stroke volume index (SVi) all rose significantly (p < 0.01 for each), with no significant changes in blood pressure or heart rate. Patients who progressed to severe AS showed a greater CAVI decline (ΔCAVI -2.90 vs. -0.67; p = 0.022) and higher Vmax (4.0 vs. 3.0 m/s; p < 0.001). ΔCAVI was the only independent predictor of severe AS progression (OR 0.51 per 1-unit decrease; 95% CI: 0.20-0.89; p = 0.013). Age and sex were not significant. CAVI and peak PG showed a modest inverse correlation (ρ = -0.35). Conclusion In dialysis patients, a marked preoperative decline in CAVI nearly doubles the risk of emergent severe AS and normalizes after valve replacement, indicating true hemodynamic responsiveness. Serial CAVI monitoring, simple, noninvasive, and reproducible, may offer an early warning signal and help optimize intervention timing when echocardiographic findings are ambiguous.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"17 9","pages":"e93263"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465358/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association Between Longitudinal Changes in Cardio-Ankle Vascular Index and Aortic Stenosis Progression in Dialysis Patients: A Retrospective Study.\",\"authors\":\"Shunsuke Todani, Kazuhiro Shimizu, Shuji Sato, Kohji Shirai, Atsuhito Saiki\",\"doi\":\"10.7759/cureus.93263\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Objective In dialysis patients, echocardiography often underestimates the progression of aortic stenosis (AS) due to blood pressure fluctuations and extensive calcification that obscure standard indices. We evaluated whether serial changes in the cardio-ankle vascular index (CAVI), a blood pressure-independent marker of arterial stiffness, can anticipate severe AS and guide the timing of valve replacement. Methods This single-center, retrospective study screened 1,169 maintenance dialysis patients (2015-2023). Forty-one patients who underwent surgical or transcatheter aortic valve replacement (AVR/TAVR) had valid CAVI measurements at four time points: 2 years and 1 year before surgery, immediately before surgery, and 1 year after surgery. The -2-year time point served as the baseline. Hemodynamic, echocardiographic, and laboratory data were analyzed using the Friedman and Wilcoxon tests. Severe AS progression was defined as a new mean pressure gradient (meanPG) ≥ 40 mmHg. Determinants of progression were identified using multivariable logistic regression. Results Median CAVI declined from 10.2 to 9.4 over the two years preceding surgery (p < 0.001) and rose to 11.1 one year post-AVR/TAVR (p < 0.001). Simultaneously, ejection time increased, ejection fraction decreased, and Vmax, maxPG, stroke volume, and stroke volume index (SVi) all rose significantly (p < 0.01 for each), with no significant changes in blood pressure or heart rate. Patients who progressed to severe AS showed a greater CAVI decline (ΔCAVI -2.90 vs. -0.67; p = 0.022) and higher Vmax (4.0 vs. 3.0 m/s; p < 0.001). ΔCAVI was the only independent predictor of severe AS progression (OR 0.51 per 1-unit decrease; 95% CI: 0.20-0.89; p = 0.013). Age and sex were not significant. CAVI and peak PG showed a modest inverse correlation (ρ = -0.35). Conclusion In dialysis patients, a marked preoperative decline in CAVI nearly doubles the risk of emergent severe AS and normalizes after valve replacement, indicating true hemodynamic responsiveness. Serial CAVI monitoring, simple, noninvasive, and reproducible, may offer an early warning signal and help optimize intervention timing when echocardiographic findings are ambiguous.</p>\",\"PeriodicalId\":93960,\"journal\":{\"name\":\"Cureus\",\"volume\":\"17 9\",\"pages\":\"e93263\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465358/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cureus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7759/cureus.93263\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.93263","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
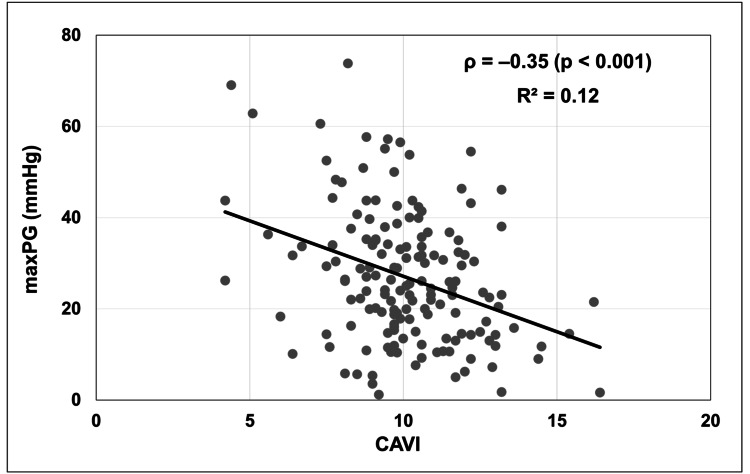
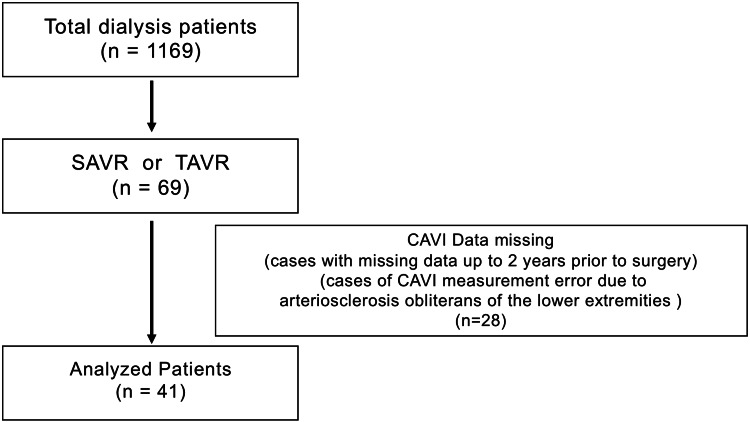
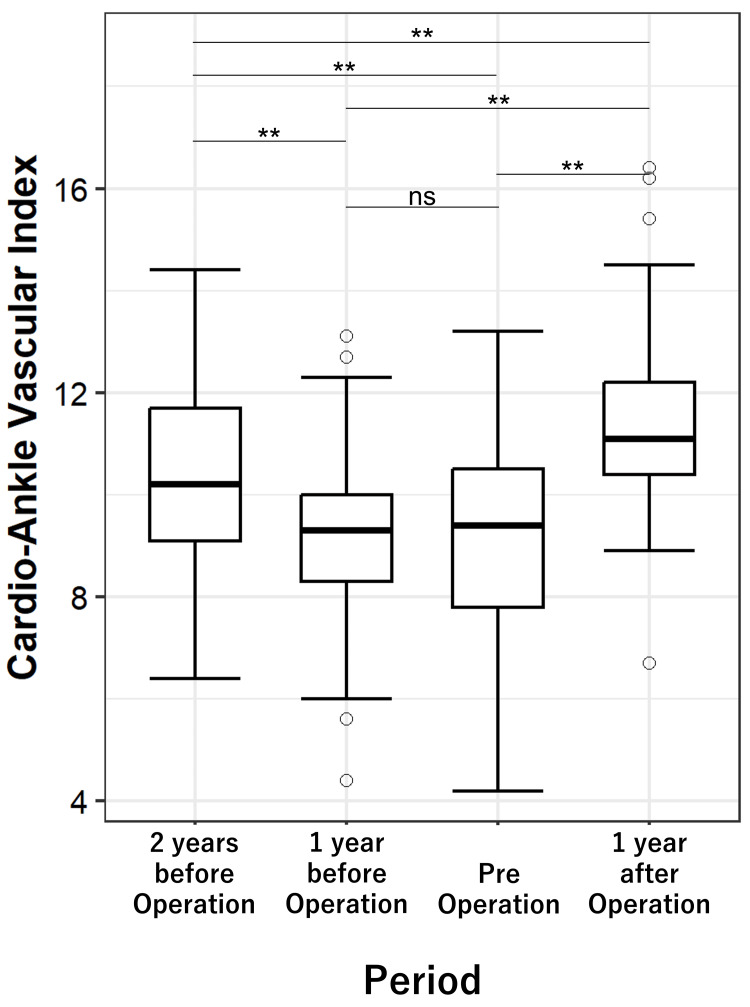
目的在透析患者中,由于血压波动和广泛钙化模糊了标准指标,超声心动图经常低估主动脉瓣狭窄(AS)的进展。我们评估了心踝血管指数(CAVI)的一系列变化是否可以预测严重的AS并指导瓣膜置换术的时机。CAVI是一种与血压无关的动脉硬度指标。方法本研究为单中心、回顾性研究,筛选2015-2023年1169例维持性透析患者。41例接受手术或经导管主动脉瓣置换术(AVR/TAVR)的患者在四个时间点(术前2年和1年、术前立即和术后1年)有有效的CAVI测量。以-2年时间点为基线。采用Friedman和Wilcoxon试验分析血流动力学、超声心动图和实验室数据。重度AS进展定义为新的平均压力梯度(mean pg)≥40 mmHg。使用多变量逻辑回归确定进展的决定因素。结果中位CAVI术前2年从10.2下降到9.4 (p < 0.001), avr /TAVR术后1年上升到11.1 (p < 0.001)。同时,射血时间增加,射血分数降低,Vmax、maxPG、卒中容积、卒中容积指数(SVi)均显著升高(p < 0.01),血压、心率无显著变化。进展为严重AS的患者CAVI下降幅度更大(ΔCAVI -2.90 vs. -0.67; p = 0.022), Vmax更高(4.0 vs. 3.0 m/s; p < 0.001)。ΔCAVI是严重AS进展的唯一独立预测因子(OR为0.51 / 1单位减少;95% CI: 0.20-0.89; p = 0.013)。年龄和性别差异不显著。CAVI与峰值PG呈适度负相关(ρ = -0.35)。结论在透析患者中,术前CAVI的显著下降使出现严重AS的风险增加近一倍,并在瓣膜置换术后恢复正常,表明真正的血流动力学反应。连续的CAVI监测,简单、无创、可重复,可提供早期预警信号,并有助于优化超声心动图结果不明确时的干预时机。
Association Between Longitudinal Changes in Cardio-Ankle Vascular Index and Aortic Stenosis Progression in Dialysis Patients: A Retrospective Study.
Objective In dialysis patients, echocardiography often underestimates the progression of aortic stenosis (AS) due to blood pressure fluctuations and extensive calcification that obscure standard indices. We evaluated whether serial changes in the cardio-ankle vascular index (CAVI), a blood pressure-independent marker of arterial stiffness, can anticipate severe AS and guide the timing of valve replacement. Methods This single-center, retrospective study screened 1,169 maintenance dialysis patients (2015-2023). Forty-one patients who underwent surgical or transcatheter aortic valve replacement (AVR/TAVR) had valid CAVI measurements at four time points: 2 years and 1 year before surgery, immediately before surgery, and 1 year after surgery. The -2-year time point served as the baseline. Hemodynamic, echocardiographic, and laboratory data were analyzed using the Friedman and Wilcoxon tests. Severe AS progression was defined as a new mean pressure gradient (meanPG) ≥ 40 mmHg. Determinants of progression were identified using multivariable logistic regression. Results Median CAVI declined from 10.2 to 9.4 over the two years preceding surgery (p < 0.001) and rose to 11.1 one year post-AVR/TAVR (p < 0.001). Simultaneously, ejection time increased, ejection fraction decreased, and Vmax, maxPG, stroke volume, and stroke volume index (SVi) all rose significantly (p < 0.01 for each), with no significant changes in blood pressure or heart rate. Patients who progressed to severe AS showed a greater CAVI decline (ΔCAVI -2.90 vs. -0.67; p = 0.022) and higher Vmax (4.0 vs. 3.0 m/s; p < 0.001). ΔCAVI was the only independent predictor of severe AS progression (OR 0.51 per 1-unit decrease; 95% CI: 0.20-0.89; p = 0.013). Age and sex were not significant. CAVI and peak PG showed a modest inverse correlation (ρ = -0.35). Conclusion In dialysis patients, a marked preoperative decline in CAVI nearly doubles the risk of emergent severe AS and normalizes after valve replacement, indicating true hemodynamic responsiveness. Serial CAVI monitoring, simple, noninvasive, and reproducible, may offer an early warning signal and help optimize intervention timing when echocardiographic findings are ambiguous.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


