Raluca Oltean, Liviu Oltean, Andreea Nelson Twakor, Teodor Horvat
{"title":"胸外科手术术前和术后影像学特征:来自单中心研究的见解。","authors":"Raluca Oltean, Liviu Oltean, Andreea Nelson Twakor, Teodor Horvat","doi":"10.25122/jml-2025-0121","DOIUrl":null,"url":null,"abstract":"<p><p>Thoracic surgery encompasses a broad spectrum of procedures with varying levels of risk. Preoperative imaging plays a critical role in evaluating anatomical pathology, but its predictive value for postoperative complications remains underexplored. This study aimed to assess whether specific radiologic features identified before surgery can predict key adverse outcomes, including ICU admission, in-hospital mortality, and length of hospital stay. We conducted a retrospective cohort study of 227 adult patients who underwent thoracic surgeries, including lobectomy, esophagectomy, thymectomy, and mediastinotomy, between 2019 and 2024. Preoperative imaging findings from chest radiographs, CT, PET-CT, MRI, and bronchoscopy were coded and analyzed. Outcomes included ICU admission, in-hospital mortality, and hospitalization duration. Univariate and multivariate logistic regressions were used to assess associations between imaging features and outcomes. Non-parametric tests and visual network plots were also applied. Common imaging findings included emphysema (29.1%), pleural effusion (12.8%), and nodules/metastases (7.9%). ICU admission occurred in 15% of patients, and in-hospital mortality occurred in 7.5%. Certain radiologic features, such as mediastinal lymphadenopathy (OR = 2.03) and nodules/metastases, showed a trend toward increased ICU admission. Conversely, features like bronchogram and no abnormalities were associated with a lower risk. Visual network analyses supported these trends. Preoperative imaging features, particularly those related to mediastinal or tumor burden, may offer predictive value for identifying patients at elevated postoperative risk. Incorporating radiologic markers into preoperative assessment could improve surgical planning and triage for intensive monitoring.</p>","PeriodicalId":16386,"journal":{"name":"Journal of Medicine and Life","volume":"18 8","pages":"794-803"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12467458/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative and postoperative imaging features in thoracic surgery: insights from a single-center study.\",\"authors\":\"Raluca Oltean, Liviu Oltean, Andreea Nelson Twakor, Teodor Horvat\",\"doi\":\"10.25122/jml-2025-0121\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Thoracic surgery encompasses a broad spectrum of procedures with varying levels of risk. Preoperative imaging plays a critical role in evaluating anatomical pathology, but its predictive value for postoperative complications remains underexplored. This study aimed to assess whether specific radiologic features identified before surgery can predict key adverse outcomes, including ICU admission, in-hospital mortality, and length of hospital stay. We conducted a retrospective cohort study of 227 adult patients who underwent thoracic surgeries, including lobectomy, esophagectomy, thymectomy, and mediastinotomy, between 2019 and 2024. Preoperative imaging findings from chest radiographs, CT, PET-CT, MRI, and bronchoscopy were coded and analyzed. Outcomes included ICU admission, in-hospital mortality, and hospitalization duration. Univariate and multivariate logistic regressions were used to assess associations between imaging features and outcomes. Non-parametric tests and visual network plots were also applied. Common imaging findings included emphysema (29.1%), pleural effusion (12.8%), and nodules/metastases (7.9%). ICU admission occurred in 15% of patients, and in-hospital mortality occurred in 7.5%. Certain radiologic features, such as mediastinal lymphadenopathy (OR = 2.03) and nodules/metastases, showed a trend toward increased ICU admission. Conversely, features like bronchogram and no abnormalities were associated with a lower risk. Visual network analyses supported these trends. Preoperative imaging features, particularly those related to mediastinal or tumor burden, may offer predictive value for identifying patients at elevated postoperative risk. Incorporating radiologic markers into preoperative assessment could improve surgical planning and triage for intensive monitoring.</p>\",\"PeriodicalId\":16386,\"journal\":{\"name\":\"Journal of Medicine and Life\",\"volume\":\"18 8\",\"pages\":\"794-803\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12467458/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medicine and Life\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25122/jml-2025-0121\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medicine and Life","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25122/jml-2025-0121","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Preoperative and postoperative imaging features in thoracic surgery: insights from a single-center study.
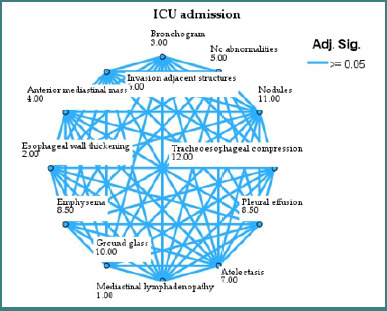
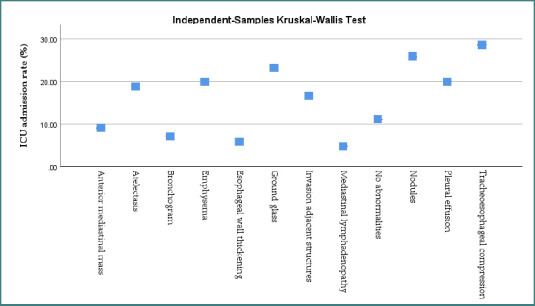
Thoracic surgery encompasses a broad spectrum of procedures with varying levels of risk. Preoperative imaging plays a critical role in evaluating anatomical pathology, but its predictive value for postoperative complications remains underexplored. This study aimed to assess whether specific radiologic features identified before surgery can predict key adverse outcomes, including ICU admission, in-hospital mortality, and length of hospital stay. We conducted a retrospective cohort study of 227 adult patients who underwent thoracic surgeries, including lobectomy, esophagectomy, thymectomy, and mediastinotomy, between 2019 and 2024. Preoperative imaging findings from chest radiographs, CT, PET-CT, MRI, and bronchoscopy were coded and analyzed. Outcomes included ICU admission, in-hospital mortality, and hospitalization duration. Univariate and multivariate logistic regressions were used to assess associations between imaging features and outcomes. Non-parametric tests and visual network plots were also applied. Common imaging findings included emphysema (29.1%), pleural effusion (12.8%), and nodules/metastases (7.9%). ICU admission occurred in 15% of patients, and in-hospital mortality occurred in 7.5%. Certain radiologic features, such as mediastinal lymphadenopathy (OR = 2.03) and nodules/metastases, showed a trend toward increased ICU admission. Conversely, features like bronchogram and no abnormalities were associated with a lower risk. Visual network analyses supported these trends. Preoperative imaging features, particularly those related to mediastinal or tumor burden, may offer predictive value for identifying patients at elevated postoperative risk. Incorporating radiologic markers into preoperative assessment could improve surgical planning and triage for intensive monitoring.
期刊介绍:
The Journal of Medicine and Life publishes peer-reviewed articles from various fields of medicine and life sciences, including original research, systematic reviews, special reports, case presentations, major medical breakthroughs and letters to the editor. The Journal focuses on current matters that lie at the intersection of biomedical science and clinical practice and strives to present this information to inform health care delivery and improve patient outcomes. Papers addressing topics such as neuroprotection, neurorehabilitation, neuroplasticity, and neuroregeneration are particularly encouraged, as part of the Journal''s continuous interest in neuroscience research. The Editorial Board of the Journal of Medicine and Life is open to consider manuscripts from all levels of research and areas of biological sciences, including fundamental, experimental or clinical research and matters of public health. As part of our pledge to promote an educational and community-building environment, our issues feature sections designated to informing our readers regarding exciting international congresses, teaching courses and relevant institutional-level events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


