Truong Phi Hung, Dang Tuong Vi, Nguyen Minh Kha, Nguyen Nhat Tai, Ly Quang Sang, Tran Hoa, Hoang Van Sy
{"title":"院外心脏骤停与ROSC的临床结果:来自越南一家专业转诊中心的见解。","authors":"Truong Phi Hung, Dang Tuong Vi, Nguyen Minh Kha, Nguyen Nhat Tai, Ly Quang Sang, Tran Hoa, Hoang Van Sy","doi":"10.5455/aim.2024.33.16-22","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anti-N-Out-of-hospital cardiac arrest (OHCA) remains a condition with high morbidity and mortality despite advancements in resuscitation strategies. Identifying prognostic factors in OHCA patients who achieve a return of spontaneous circulation (ROSC) is critical for optimizing post-resuscitation care and improving survival outcomes.</p><p><strong>Objective: </strong>This study evaluates clinical outcomes and predictors of in-hospital mortality in OHCA patients admitted to a tertiary referral center in Southern Vietnam.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted on OHCA patients with ROSC admitted to Cho Ray Hospital, Ho Chi Minh City, Vietnam, from January 1, 2019, to June 15, 2024. Demographic characteristics, clinical variables, and survival outcomes were analyzed. Predictors of in-hospital mortality were identified through multivariate logistic regression.</p><p><strong>Results: </strong>Among 482 OHCA cases, 86 patients met the inclusion criteria. The mean age was 49.1 ± 17.2 years, with a male predominance (79.1%, male-to-female ratio: 3.8:1). Most cardiac arrests were witnessed (84.9%), and 32.5% presented with an initial shockable rhythm. Cardiac etiology was the predominant cause (67.4%). The overall in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (Cerebral Performance Category [CPC] 1-2). Multivariate analysis identified lower Glasgow Coma Scale (GCS) scores (OR 1.42, 95% CI 1.01-2.00, p = 0.045), decreased estimated glomerular filtration rate (eGFR) (OR 1.03, 95% CI 1.00-1.06, p = 0.042), and higher cumulative epinephrine dose (OR 1.10, 95% CI 1.01-1.19, p < 0.05) as independent predictors of mortality. A predictive model incorporating these variables demonstrated strong discriminatory performance (AUC = 0.91). An epinephrine threshold of 7 mg was identified as a predictor of in-hospital mortality, with a sensitivity of 0.68 and specificity of 0.91.</p><p><strong>Conclusion: </strong>In OHCA patients with ROSC, the in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (CPC 1-2). Lower GCS scores, reduced eGFR, and higher total epinephrine doses were independently associated with increased mortality. These findings underscore the need for early risk stratification and individualized post-resuscitation management to improve patient outcomes.</p>","PeriodicalId":7074,"journal":{"name":"Acta Informatica Medica","volume":"33 1","pages":"16-22"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12464537/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes of Out-of-Hospital Cardiac Arrest with ROSC: Insights from a Specialized Referral Center in Vietnam.\",\"authors\":\"Truong Phi Hung, Dang Tuong Vi, Nguyen Minh Kha, Nguyen Nhat Tai, Ly Quang Sang, Tran Hoa, Hoang Van Sy\",\"doi\":\"10.5455/aim.2024.33.16-22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Anti-N-Out-of-hospital cardiac arrest (OHCA) remains a condition with high morbidity and mortality despite advancements in resuscitation strategies. Identifying prognostic factors in OHCA patients who achieve a return of spontaneous circulation (ROSC) is critical for optimizing post-resuscitation care and improving survival outcomes.</p><p><strong>Objective: </strong>This study evaluates clinical outcomes and predictors of in-hospital mortality in OHCA patients admitted to a tertiary referral center in Southern Vietnam.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted on OHCA patients with ROSC admitted to Cho Ray Hospital, Ho Chi Minh City, Vietnam, from January 1, 2019, to June 15, 2024. Demographic characteristics, clinical variables, and survival outcomes were analyzed. Predictors of in-hospital mortality were identified through multivariate logistic regression.</p><p><strong>Results: </strong>Among 482 OHCA cases, 86 patients met the inclusion criteria. The mean age was 49.1 ± 17.2 years, with a male predominance (79.1%, male-to-female ratio: 3.8:1). Most cardiac arrests were witnessed (84.9%), and 32.5% presented with an initial shockable rhythm. Cardiac etiology was the predominant cause (67.4%). The overall in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (Cerebral Performance Category [CPC] 1-2). Multivariate analysis identified lower Glasgow Coma Scale (GCS) scores (OR 1.42, 95% CI 1.01-2.00, p = 0.045), decreased estimated glomerular filtration rate (eGFR) (OR 1.03, 95% CI 1.00-1.06, p = 0.042), and higher cumulative epinephrine dose (OR 1.10, 95% CI 1.01-1.19, p < 0.05) as independent predictors of mortality. A predictive model incorporating these variables demonstrated strong discriminatory performance (AUC = 0.91). An epinephrine threshold of 7 mg was identified as a predictor of in-hospital mortality, with a sensitivity of 0.68 and specificity of 0.91.</p><p><strong>Conclusion: </strong>In OHCA patients with ROSC, the in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (CPC 1-2). Lower GCS scores, reduced eGFR, and higher total epinephrine doses were independently associated with increased mortality. These findings underscore the need for early risk stratification and individualized post-resuscitation management to improve patient outcomes.</p>\",\"PeriodicalId\":7074,\"journal\":{\"name\":\"Acta Informatica Medica\",\"volume\":\"33 1\",\"pages\":\"16-22\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12464537/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Informatica Medica\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5455/aim.2024.33.16-22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Informatica Medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5455/aim.2024.33.16-22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:院外抗n型心脏骤停(OHCA)仍然是一种高发病率和死亡率的疾病,尽管复苏策略有所进步。确定实现自然循环恢复(ROSC)的OHCA患者的预后因素对于优化复苏后护理和改善生存结果至关重要。目的:本研究评估越南南部一家三级转诊中心收治的OHCA患者的临床结局和住院死亡率预测因素。方法:对2019年1月1日至2024年6月15日在越南胡志明市Cho Ray医院住院的OHCA合并ROSC患者进行回顾性队列研究。分析人口学特征、临床变量和生存结果。通过多变量logistic回归确定住院死亡率的预测因素。结果:482例OHCA患者中,86例符合纳入标准。平均年龄49.1±17.2岁,男性居多(79.1%),男女比例为3.8:1。大多数心脏骤停(84.9%),32.5%表现为最初的休克性心律。心脏病因占主要原因(67.4%)。总体住院生存率为44.2%,其中25.6%获得良好的神经预后(脑功能分类[CPC] 1-2)。多因素分析发现,较低的格拉斯哥昏迷量表评分(GCS) (OR 1.42, 95% CI 1.01-2.00, p = 0.045)、较低的肾小球滤过率(eGFR) (OR 1.03, 95% CI 1.00-1.06, p = 0.042)和较高的累积肾上腺素剂量(OR 1.10, 95% CI 1.01-1.19, p < 0.05)是死亡率的独立预测因子。纳入这些变量的预测模型显示出很强的歧视性表现(AUC = 0.91)。7 mg肾上腺素阈值被确定为住院死亡率的预测因子,敏感性为0.68,特异性为0.91。结论:OHCA合并ROSC患者的住院生存率为44.2%,其中25.6%获得良好的神经预后(CPC 1-2)。较低的GCS评分、降低的eGFR和较高的总肾上腺素剂量与死亡率增加独立相关。这些发现强调了早期风险分层和个性化复苏后管理的必要性,以改善患者的预后。
Clinical Outcomes of Out-of-Hospital Cardiac Arrest with ROSC: Insights from a Specialized Referral Center in Vietnam.
Background: Anti-N-Out-of-hospital cardiac arrest (OHCA) remains a condition with high morbidity and mortality despite advancements in resuscitation strategies. Identifying prognostic factors in OHCA patients who achieve a return of spontaneous circulation (ROSC) is critical for optimizing post-resuscitation care and improving survival outcomes.
Objective: This study evaluates clinical outcomes and predictors of in-hospital mortality in OHCA patients admitted to a tertiary referral center in Southern Vietnam.
Methods: A retrospective cohort study was conducted on OHCA patients with ROSC admitted to Cho Ray Hospital, Ho Chi Minh City, Vietnam, from January 1, 2019, to June 15, 2024. Demographic characteristics, clinical variables, and survival outcomes were analyzed. Predictors of in-hospital mortality were identified through multivariate logistic regression.
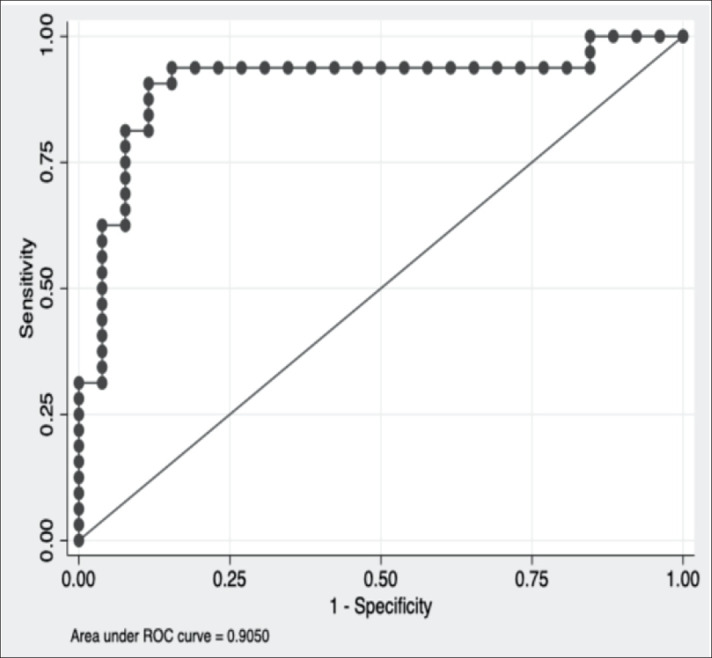
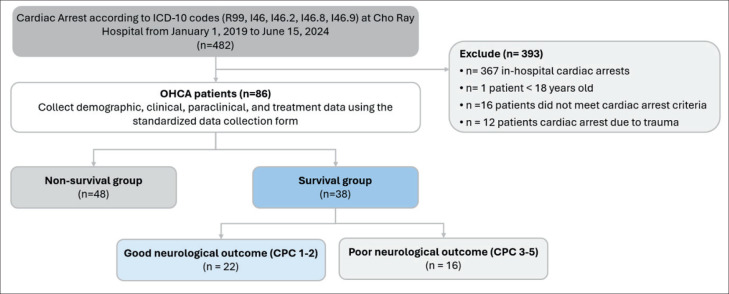
Results: Among 482 OHCA cases, 86 patients met the inclusion criteria. The mean age was 49.1 ± 17.2 years, with a male predominance (79.1%, male-to-female ratio: 3.8:1). Most cardiac arrests were witnessed (84.9%), and 32.5% presented with an initial shockable rhythm. Cardiac etiology was the predominant cause (67.4%). The overall in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (Cerebral Performance Category [CPC] 1-2). Multivariate analysis identified lower Glasgow Coma Scale (GCS) scores (OR 1.42, 95% CI 1.01-2.00, p = 0.045), decreased estimated glomerular filtration rate (eGFR) (OR 1.03, 95% CI 1.00-1.06, p = 0.042), and higher cumulative epinephrine dose (OR 1.10, 95% CI 1.01-1.19, p < 0.05) as independent predictors of mortality. A predictive model incorporating these variables demonstrated strong discriminatory performance (AUC = 0.91). An epinephrine threshold of 7 mg was identified as a predictor of in-hospital mortality, with a sensitivity of 0.68 and specificity of 0.91.
Conclusion: In OHCA patients with ROSC, the in-hospital survival rate was 44.2%, with 25.6% achieving good neurological outcomes (CPC 1-2). Lower GCS scores, reduced eGFR, and higher total epinephrine doses were independently associated with increased mortality. These findings underscore the need for early risk stratification and individualized post-resuscitation management to improve patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


