{"title":"先前经皮冠状动脉介入治疗的解剖负担和冠状动脉旁路移植术后的长期结果:一项跨越二十年的分析。","authors":"Go Yamashita, Jiro Sakai, Takumi Takauchi, Shun Otani, Shoya Nakano, Ryo Fujimoto, Atsushi Sugaya, Shingo Hirao, Tatsuhiko Komiya","doi":"10.1093/icvts/ivaf237","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aimed to determine whether the anatomical burden of prior percutaneous coronary intervention(PCI) influences long-term outcomes after coronary artery bypass grafting, beyond the impact of intervention presence alone.</p><p><strong>Methods: </strong>This retrospective study analyzed consecutive patients undergoing coronary artery bypass grafting at a single institution between 2000 and 2024. The inclusion criteria comprised isolated, non-emergent surgery. Patient categorization was based on prior PCI-treated lesions: none, single, or multiple. The primary endpoint was long-term overall survival. The secondary endpoints included cardiac death, myocardial infarction, stroke, heart failure hospitalization, and repeat revascularization. Long-term outcomes were assessed using Kaplan-Meier analysis and Cox multivariable models, adjusting for 26 clinical factors.</p><p><strong>Results: </strong>Of 2,442 patients, 1,205 met the inclusion criteria (755 none, 227 single-lesion, 223 multiple-lesion intervention). Over a median follow-up of 12.0 (interquartile range, 11.3-12.9; maximum: 24.2) years, the multiple-lesion intervention group had higher rates of in-hospital acute kidney injury (34.1% vs. 21.1% vs. 24.2%, P = 0.003). Overall survival differed significantly between groups over the follow-up period (log-rank P = 0.004), with 15-year survival rates of 35.8%, 46.0%, and 48.0% for multiple-lesion, single-lesion, and no prior PCI groups, respectively. After adjustment, multiple-lesion intervention was associated with increased risks of cardiac death (adjusted subdistribution hazard ratio: 1.91), myocardial infarction (2.26), and repeat revascularization (1.92) compared with no prior intervention.</p><p><strong>Conclusions: </strong>Multiple-lesion PCI was associated with higher long-term risks of cardiac death, myocardial infarction, and repeat revascularization, while stroke risk was similar. Single-lesion PCI showed outcomes comparable to no prior PCI except for higher heart failure hospitalization. These findings require confirmation in larger, multicenter comparative studies to address residual confounding.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12516811/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anatomical burden of prior percutaneous coronary intervention and long-term outcomes after coronary artery bypass grafting: An analysis spanning two decades.\",\"authors\":\"Go Yamashita, Jiro Sakai, Takumi Takauchi, Shun Otani, Shoya Nakano, Ryo Fujimoto, Atsushi Sugaya, Shingo Hirao, Tatsuhiko Komiya\",\"doi\":\"10.1093/icvts/ivaf237\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This study aimed to determine whether the anatomical burden of prior percutaneous coronary intervention(PCI) influences long-term outcomes after coronary artery bypass grafting, beyond the impact of intervention presence alone.</p><p><strong>Methods: </strong>This retrospective study analyzed consecutive patients undergoing coronary artery bypass grafting at a single institution between 2000 and 2024. The inclusion criteria comprised isolated, non-emergent surgery. Patient categorization was based on prior PCI-treated lesions: none, single, or multiple. The primary endpoint was long-term overall survival. The secondary endpoints included cardiac death, myocardial infarction, stroke, heart failure hospitalization, and repeat revascularization. Long-term outcomes were assessed using Kaplan-Meier analysis and Cox multivariable models, adjusting for 26 clinical factors.</p><p><strong>Results: </strong>Of 2,442 patients, 1,205 met the inclusion criteria (755 none, 227 single-lesion, 223 multiple-lesion intervention). Over a median follow-up of 12.0 (interquartile range, 11.3-12.9; maximum: 24.2) years, the multiple-lesion intervention group had higher rates of in-hospital acute kidney injury (34.1% vs. 21.1% vs. 24.2%, P = 0.003). Overall survival differed significantly between groups over the follow-up period (log-rank P = 0.004), with 15-year survival rates of 35.8%, 46.0%, and 48.0% for multiple-lesion, single-lesion, and no prior PCI groups, respectively. After adjustment, multiple-lesion intervention was associated with increased risks of cardiac death (adjusted subdistribution hazard ratio: 1.91), myocardial infarction (2.26), and repeat revascularization (1.92) compared with no prior intervention.</p><p><strong>Conclusions: </strong>Multiple-lesion PCI was associated with higher long-term risks of cardiac death, myocardial infarction, and repeat revascularization, while stroke risk was similar. Single-lesion PCI showed outcomes comparable to no prior PCI except for higher heart failure hospitalization. These findings require confirmation in larger, multicenter comparative studies to address residual confounding.</p>\",\"PeriodicalId\":73406,\"journal\":{\"name\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12516811/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivaf237\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf237","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究旨在确定先前经皮冠状动脉介入治疗(PCI)的解剖负担是否会影响冠状动脉旁路移植术后的长期预后,而不仅仅是干预存在的影响。方法:本回顾性研究分析了2000年至2024年间在同一家机构连续接受冠状动脉旁路移植术的患者。纳入标准包括孤立的非紧急手术。患者分类基于先前pci治疗的病变:无,单一或多个。主要终点是长期总生存期。次要终点包括心源性死亡、心肌梗死、中风、心力衰竭住院和重复血运重建术。采用Kaplan-Meier分析和Cox多变量模型对26个临床因素进行调整,评估长期结果。结果:2442例患者中,1205例符合纳入标准(755例无纳入,227例单灶干预,223例多灶干预)。中位随访时间为12.0年(四分位间距为11.3-12.9年,最长为24.2年),多病变干预组住院急性肾损伤发生率更高(34.1% vs. 21.1% vs. 24.2%, P = 0.003)。在随访期间,两组患者的总生存率差异显著(log-rank P = 0.004),多病变组、单病变组和无术前PCI组的15年生存率分别为35.8%、46.0%和48.0%。调整后,与未进行干预相比,多病变干预与心源性死亡(调整后亚分布风险比:1.91)、心肌梗死(2.26)和重复血运重建术(1.92)的风险增加相关。结论:多病变PCI与心源性死亡、心肌梗死和重复血运重建术的长期风险较高相关,而卒中风险相似。除了心力衰竭住院率较高外,单病灶PCI显示的结果与没有术前PCI相当。这些发现需要在更大的、多中心的比较研究中得到证实,以解决残留的混杂因素。
Anatomical burden of prior percutaneous coronary intervention and long-term outcomes after coronary artery bypass grafting: An analysis spanning two decades.
Objectives: This study aimed to determine whether the anatomical burden of prior percutaneous coronary intervention(PCI) influences long-term outcomes after coronary artery bypass grafting, beyond the impact of intervention presence alone.
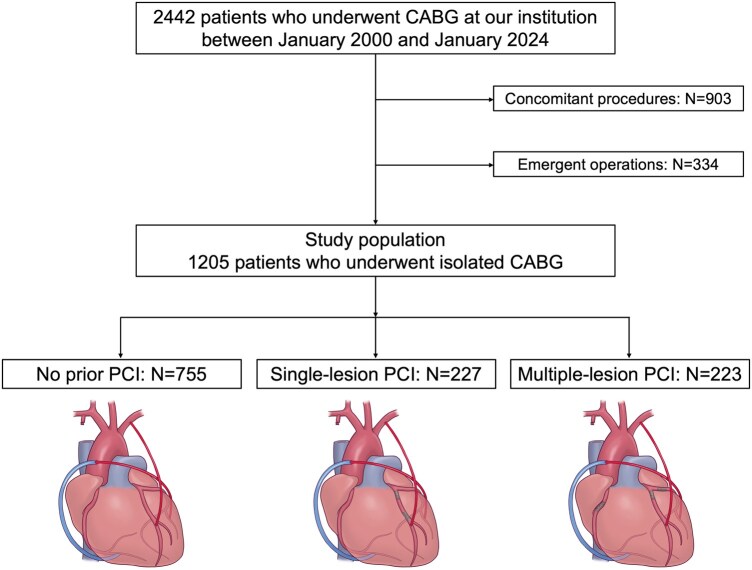
Methods: This retrospective study analyzed consecutive patients undergoing coronary artery bypass grafting at a single institution between 2000 and 2024. The inclusion criteria comprised isolated, non-emergent surgery. Patient categorization was based on prior PCI-treated lesions: none, single, or multiple. The primary endpoint was long-term overall survival. The secondary endpoints included cardiac death, myocardial infarction, stroke, heart failure hospitalization, and repeat revascularization. Long-term outcomes were assessed using Kaplan-Meier analysis and Cox multivariable models, adjusting for 26 clinical factors.
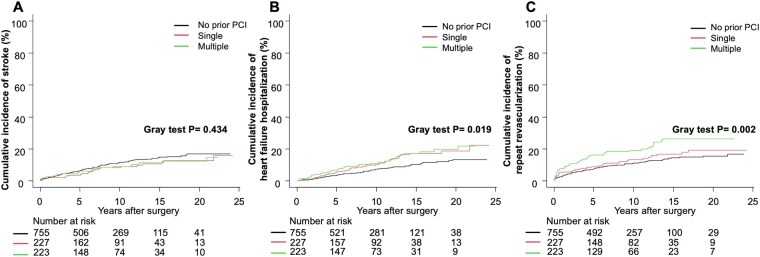
Results: Of 2,442 patients, 1,205 met the inclusion criteria (755 none, 227 single-lesion, 223 multiple-lesion intervention). Over a median follow-up of 12.0 (interquartile range, 11.3-12.9; maximum: 24.2) years, the multiple-lesion intervention group had higher rates of in-hospital acute kidney injury (34.1% vs. 21.1% vs. 24.2%, P = 0.003). Overall survival differed significantly between groups over the follow-up period (log-rank P = 0.004), with 15-year survival rates of 35.8%, 46.0%, and 48.0% for multiple-lesion, single-lesion, and no prior PCI groups, respectively. After adjustment, multiple-lesion intervention was associated with increased risks of cardiac death (adjusted subdistribution hazard ratio: 1.91), myocardial infarction (2.26), and repeat revascularization (1.92) compared with no prior intervention.
Conclusions: Multiple-lesion PCI was associated with higher long-term risks of cardiac death, myocardial infarction, and repeat revascularization, while stroke risk was similar. Single-lesion PCI showed outcomes comparable to no prior PCI except for higher heart failure hospitalization. These findings require confirmation in larger, multicenter comparative studies to address residual confounding.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


