Ci-Wen Luo, Meng-Hao Chang, Lan Lin, Frank Cheau-Feng Lin, Shih-Wei Chen, Yu-Hsiang Kuan, Pei-Chi Tsai, Ji-Kuen Yu, Stella Chin-Shaw Tsai
{"title":"甲状腺癌切除术后的长期生存率:一项倾向匹配的TriNetX研究和专业分层分析。","authors":"Ci-Wen Luo, Meng-Hao Chang, Lan Lin, Frank Cheau-Feng Lin, Shih-Wei Chen, Yu-Hsiang Kuan, Pei-Chi Tsai, Ji-Kuen Yu, Stella Chin-Shaw Tsai","doi":"10.3390/cancers17183051","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>Whether thyroidectomy confers a long-term survival advantage over non-surgical management in real-world practice remains uncertain. We primarily evaluated the association between surgery and all-cause mortality in thyroid cancer; specialty-stratified outcomes were prespecified as secondary, exploratory analyses.</p><p><strong>Methods: </strong>Using the TriNetX US Collaborative Network (2008-2024), we identified adults with thyroid cancer and created 1:1 propensity score-matched cohorts of patients who did or did not undergo thyroidectomy, balancing demographics, comorbidities, medications, and laboratory variables. Overall survival was assessed with Kaplan-Meier curves and Cox proportional hazard models. Among the surgical patients, we performed exploratory analyses stratified by operating specialty (otolaryngology-head and neck surgery (reference) vs. general/endocrine surgery and other/unknown, reported descriptively).</p><p><strong>Results: </strong>After matching, 49,219 patients were included per cohort. Thyroidectomy was associated with lower long-term mortality versus non-surgical care (adjusted HR 0.685, 95% CI 0.652-0.721). Among the surgical patients, secondary, exploratory specialty-stratified analyses suggested differences: compared with otolaryngology-head and neck surgery (ENT-HNS; reference), general/endocrine surgery (GS/ES) had a lower adjusted hazard of death (aHR 0.561, 95% CI 0.481-0.654), whereas other/unknown specialties had a higher adjusted hazard (aHR 1.583, 95% CI 1.302-1.924). These patterns are hypothesis-generating and may reflect residual confounding, including the tumor stage and histology, referral pathways, and surgeon or center experience.</p><p><strong>Conclusions: </strong>In a large, propensity-matched real-world cohort, surgery was linked to improved long-term survival regarding thyroid cancer. Observed specialty-related variation should be interpreted cautiously, and prospective studies incorporating tumor-level variables and provider/center characteristics are needed. Emphasis should remain on timely surgery within multidisciplinary care pathways.</p>","PeriodicalId":9681,"journal":{"name":"Cancers","volume":"17 18","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468916/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-Term Survival After Thyroidectomy for Thyroid Cancer: A Propensity-Matched TriNetX Study with Specialty-Stratified Analyses.\",\"authors\":\"Ci-Wen Luo, Meng-Hao Chang, Lan Lin, Frank Cheau-Feng Lin, Shih-Wei Chen, Yu-Hsiang Kuan, Pei-Chi Tsai, Ji-Kuen Yu, Stella Chin-Shaw Tsai\",\"doi\":\"10.3390/cancers17183051\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/objectives: </strong>Whether thyroidectomy confers a long-term survival advantage over non-surgical management in real-world practice remains uncertain. We primarily evaluated the association between surgery and all-cause mortality in thyroid cancer; specialty-stratified outcomes were prespecified as secondary, exploratory analyses.</p><p><strong>Methods: </strong>Using the TriNetX US Collaborative Network (2008-2024), we identified adults with thyroid cancer and created 1:1 propensity score-matched cohorts of patients who did or did not undergo thyroidectomy, balancing demographics, comorbidities, medications, and laboratory variables. Overall survival was assessed with Kaplan-Meier curves and Cox proportional hazard models. Among the surgical patients, we performed exploratory analyses stratified by operating specialty (otolaryngology-head and neck surgery (reference) vs. general/endocrine surgery and other/unknown, reported descriptively).</p><p><strong>Results: </strong>After matching, 49,219 patients were included per cohort. Thyroidectomy was associated with lower long-term mortality versus non-surgical care (adjusted HR 0.685, 95% CI 0.652-0.721). Among the surgical patients, secondary, exploratory specialty-stratified analyses suggested differences: compared with otolaryngology-head and neck surgery (ENT-HNS; reference), general/endocrine surgery (GS/ES) had a lower adjusted hazard of death (aHR 0.561, 95% CI 0.481-0.654), whereas other/unknown specialties had a higher adjusted hazard (aHR 1.583, 95% CI 1.302-1.924). These patterns are hypothesis-generating and may reflect residual confounding, including the tumor stage and histology, referral pathways, and surgeon or center experience.</p><p><strong>Conclusions: </strong>In a large, propensity-matched real-world cohort, surgery was linked to improved long-term survival regarding thyroid cancer. Observed specialty-related variation should be interpreted cautiously, and prospective studies incorporating tumor-level variables and provider/center characteristics are needed. Emphasis should remain on timely surgery within multidisciplinary care pathways.</p>\",\"PeriodicalId\":9681,\"journal\":{\"name\":\"Cancers\",\"volume\":\"17 18\",\"pages\":\"\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468916/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancers\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/cancers17183051\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/cancers17183051","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景/目的:在现实世界的实践中,甲状腺切除术是否比非手术治疗具有长期生存优势仍不确定。我们主要评估甲状腺癌手术与全因死亡率之间的关系;专业分层的结果被预先指定为次要的探索性分析。方法:使用TriNetX美国合作网络(2008-2024),我们确定了患有甲状腺癌的成年人,并创建了1:1倾向评分匹配的队列,这些患者接受或未接受甲状腺切除术,平衡人口统计学、合并症、药物和实验室变量。采用Kaplan-Meier曲线和Cox比例风险模型评估总生存率。在手术患者中,我们按手术专业(耳鼻喉-头颈外科(参考)与普通/内分泌外科和其他/未知,描述性报道)分层进行了探索性分析。结果:匹配后,每个队列纳入49,219例患者。与非手术治疗相比,甲状腺切除术与较低的长期死亡率相关(校正HR 0.685, 95% CI 0.652-0.721)。在手术患者中,二级、探索性专业分层分析显示差异:与耳鼻喉头颈外科(nt - hns; reference)相比,普通/内分泌外科(GS/ES)的调整死亡风险较低(aHR 0.561, 95% CI 0.481-0.654),而其他/未知专业的调整死亡风险较高(aHR 1.583, 95% CI 1.304 -1.924)。这些模式是假设产生的,可能反映残留的混杂因素,包括肿瘤分期和组织学、转诊途径、外科医生或中心经验。结论:在一个大的、倾向匹配的现实世界队列中,手术与甲状腺癌患者长期生存率的提高有关。观察到的专科相关变异应谨慎解释,需要前瞻性研究结合肿瘤水平变量和提供者/中心特征。重点仍应放在多学科护理途径中的及时手术上。
Long-Term Survival After Thyroidectomy for Thyroid Cancer: A Propensity-Matched TriNetX Study with Specialty-Stratified Analyses.
Background/objectives: Whether thyroidectomy confers a long-term survival advantage over non-surgical management in real-world practice remains uncertain. We primarily evaluated the association between surgery and all-cause mortality in thyroid cancer; specialty-stratified outcomes were prespecified as secondary, exploratory analyses.
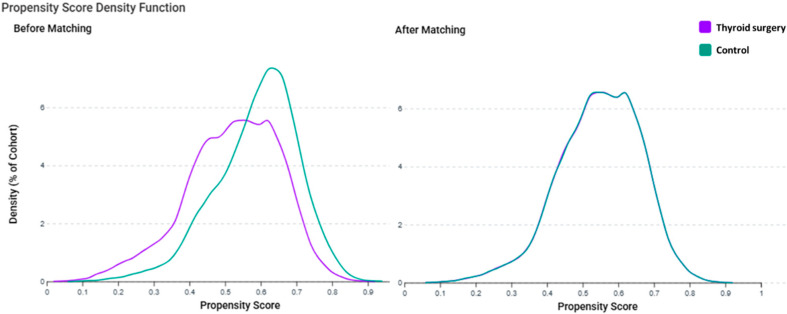
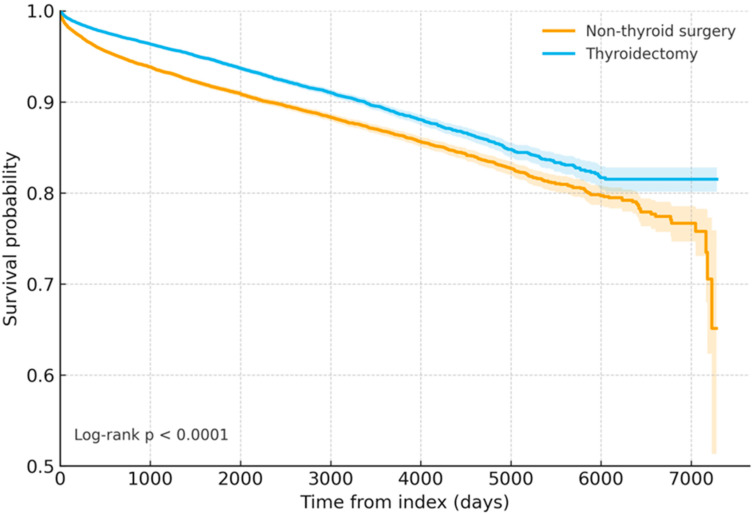
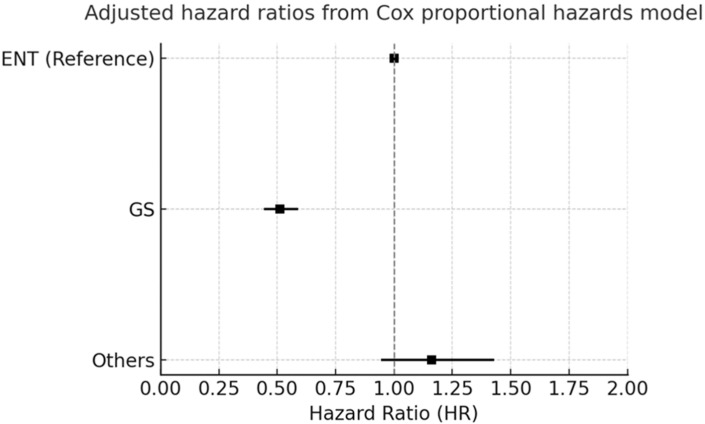
Methods: Using the TriNetX US Collaborative Network (2008-2024), we identified adults with thyroid cancer and created 1:1 propensity score-matched cohorts of patients who did or did not undergo thyroidectomy, balancing demographics, comorbidities, medications, and laboratory variables. Overall survival was assessed with Kaplan-Meier curves and Cox proportional hazard models. Among the surgical patients, we performed exploratory analyses stratified by operating specialty (otolaryngology-head and neck surgery (reference) vs. general/endocrine surgery and other/unknown, reported descriptively).
Results: After matching, 49,219 patients were included per cohort. Thyroidectomy was associated with lower long-term mortality versus non-surgical care (adjusted HR 0.685, 95% CI 0.652-0.721). Among the surgical patients, secondary, exploratory specialty-stratified analyses suggested differences: compared with otolaryngology-head and neck surgery (ENT-HNS; reference), general/endocrine surgery (GS/ES) had a lower adjusted hazard of death (aHR 0.561, 95% CI 0.481-0.654), whereas other/unknown specialties had a higher adjusted hazard (aHR 1.583, 95% CI 1.302-1.924). These patterns are hypothesis-generating and may reflect residual confounding, including the tumor stage and histology, referral pathways, and surgeon or center experience.
Conclusions: In a large, propensity-matched real-world cohort, surgery was linked to improved long-term survival regarding thyroid cancer. Observed specialty-related variation should be interpreted cautiously, and prospective studies incorporating tumor-level variables and provider/center characteristics are needed. Emphasis should remain on timely surgery within multidisciplinary care pathways.
期刊介绍:
Cancers (ISSN 2072-6694) is an international, peer-reviewed open access journal on oncology. It publishes reviews, regular research papers and short communications. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


