Ana M Moser, Michael Wang, Ava Zamani, Sabir Meah, Stephanie Daignault-Newton, Corinne Labardee, Nicholas Dybas, Jacob Clapper, Brian R Lane, Tudor Borza, Alice Semerjian, Vincent J Gnanapragasam, Kevin B Ginsburg
{"title":"STRATCANS标准在MUSIC前列腺癌主动监测队列中的应用:迈向风险分层主动监测的一步。","authors":"Ana M Moser, Michael Wang, Ava Zamani, Sabir Meah, Stephanie Daignault-Newton, Corinne Labardee, Nicholas Dybas, Jacob Clapper, Brian R Lane, Tudor Borza, Alice Semerjian, Vincent J Gnanapragasam, Kevin B Ginsburg","doi":"10.3390/cancers17183032","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The STRATified CANcer Surveillance (STRATCANS) model risk-stratifies patients with prostate cancer (PC) on active surveillance (AS) into three tiers based on their risk of disease progression. We applied STRATCANS to the Michigan Urological Surgery Improvement Collaborative (MUSIC) Prostate registry to assess its association with the risk of biopsy upgrading and time to definitive treatment in a diverse, real-world AS cohort.</p><p><strong>Methods: </strong>We retrospectively reviewed the MUSIC registry for PC patients on AS from 2016 to 2022 and classified patients by STRATCANS tier. Primary outcomes included biopsy upgrading to ≥Grade Group 3 (≥GG3), any biopsy upgrading, and time to definitive treatment.</p><p><strong>Results: </strong>Among 7578 men on AS, 4009, 2732, and 837 patients were in STRATCANS 1, 2, and 3, respectively. The risk of progression to ≥GG3 was 13%, 33%, and 53% for patients in STRATCANS 1, 2, and 3, respectively (<i>p</i> < 0.001). The rate of any biopsy upgrading was approximately 50% at 3 years across all STRATCANS tiers. STRATCANS tiers were also significantly associated with time to definitive treatment, with 16%, 28%, and 35% of men in STRATCANS 1, 2, and 3, respectively, receiving definitive treatment by 36 months. Limitations include confounding inherent to retrospective registry studies, a short 60-month follow-up period, and variability in biopsy method with no centralized pathology and radiology review.</p><p><strong>Conclusions: </strong>STRATCANS has a stepwise association with the risk of progression to ≥GG3 disease and time to definitive treatment among men on AS in the MUSIC cohort, supporting its use as a risk-based, follow-up approach in men on AS.</p>","PeriodicalId":9681,"journal":{"name":"Cancers","volume":"17 18","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468819/pdf/","citationCount":"0","resultStr":"{\"title\":\"Application of the STRATCANS Criteria to the MUSIC Prostate Cancer Active Surveillance Cohort: A Step Towards Risk-Stratified Active Surveillance.\",\"authors\":\"Ana M Moser, Michael Wang, Ava Zamani, Sabir Meah, Stephanie Daignault-Newton, Corinne Labardee, Nicholas Dybas, Jacob Clapper, Brian R Lane, Tudor Borza, Alice Semerjian, Vincent J Gnanapragasam, Kevin B Ginsburg\",\"doi\":\"10.3390/cancers17183032\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The STRATified CANcer Surveillance (STRATCANS) model risk-stratifies patients with prostate cancer (PC) on active surveillance (AS) into three tiers based on their risk of disease progression. We applied STRATCANS to the Michigan Urological Surgery Improvement Collaborative (MUSIC) Prostate registry to assess its association with the risk of biopsy upgrading and time to definitive treatment in a diverse, real-world AS cohort.</p><p><strong>Methods: </strong>We retrospectively reviewed the MUSIC registry for PC patients on AS from 2016 to 2022 and classified patients by STRATCANS tier. Primary outcomes included biopsy upgrading to ≥Grade Group 3 (≥GG3), any biopsy upgrading, and time to definitive treatment.</p><p><strong>Results: </strong>Among 7578 men on AS, 4009, 2732, and 837 patients were in STRATCANS 1, 2, and 3, respectively. The risk of progression to ≥GG3 was 13%, 33%, and 53% for patients in STRATCANS 1, 2, and 3, respectively (<i>p</i> < 0.001). The rate of any biopsy upgrading was approximately 50% at 3 years across all STRATCANS tiers. STRATCANS tiers were also significantly associated with time to definitive treatment, with 16%, 28%, and 35% of men in STRATCANS 1, 2, and 3, respectively, receiving definitive treatment by 36 months. Limitations include confounding inherent to retrospective registry studies, a short 60-month follow-up period, and variability in biopsy method with no centralized pathology and radiology review.</p><p><strong>Conclusions: </strong>STRATCANS has a stepwise association with the risk of progression to ≥GG3 disease and time to definitive treatment among men on AS in the MUSIC cohort, supporting its use as a risk-based, follow-up approach in men on AS.</p>\",\"PeriodicalId\":9681,\"journal\":{\"name\":\"Cancers\",\"volume\":\"17 18\",\"pages\":\"\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468819/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancers\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/cancers17183032\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/cancers17183032","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Application of the STRATCANS Criteria to the MUSIC Prostate Cancer Active Surveillance Cohort: A Step Towards Risk-Stratified Active Surveillance.
Background: The STRATified CANcer Surveillance (STRATCANS) model risk-stratifies patients with prostate cancer (PC) on active surveillance (AS) into three tiers based on their risk of disease progression. We applied STRATCANS to the Michigan Urological Surgery Improvement Collaborative (MUSIC) Prostate registry to assess its association with the risk of biopsy upgrading and time to definitive treatment in a diverse, real-world AS cohort.
Methods: We retrospectively reviewed the MUSIC registry for PC patients on AS from 2016 to 2022 and classified patients by STRATCANS tier. Primary outcomes included biopsy upgrading to ≥Grade Group 3 (≥GG3), any biopsy upgrading, and time to definitive treatment.
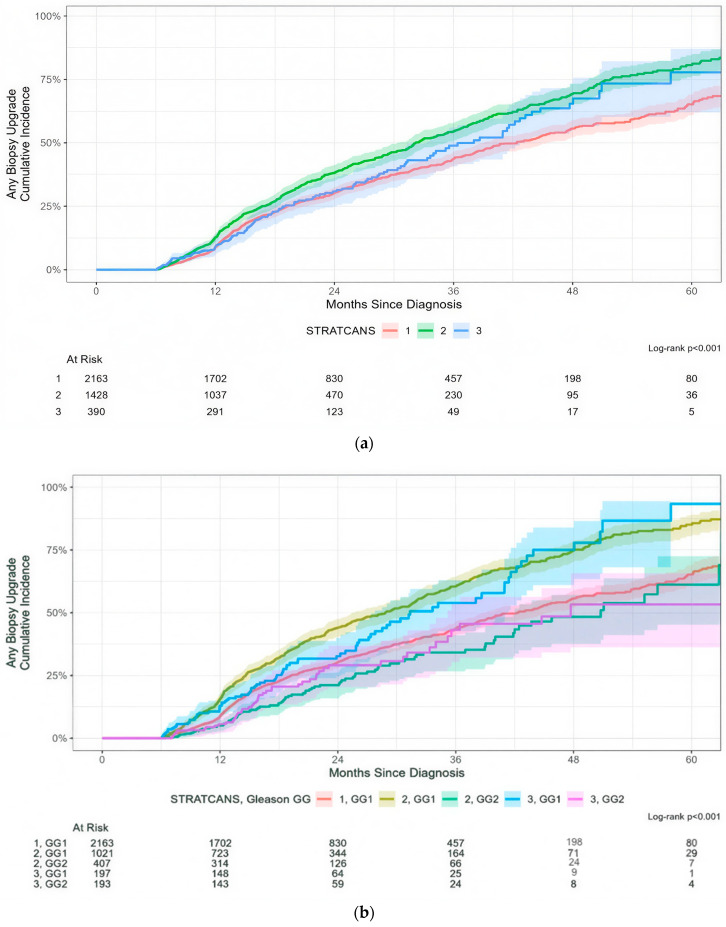
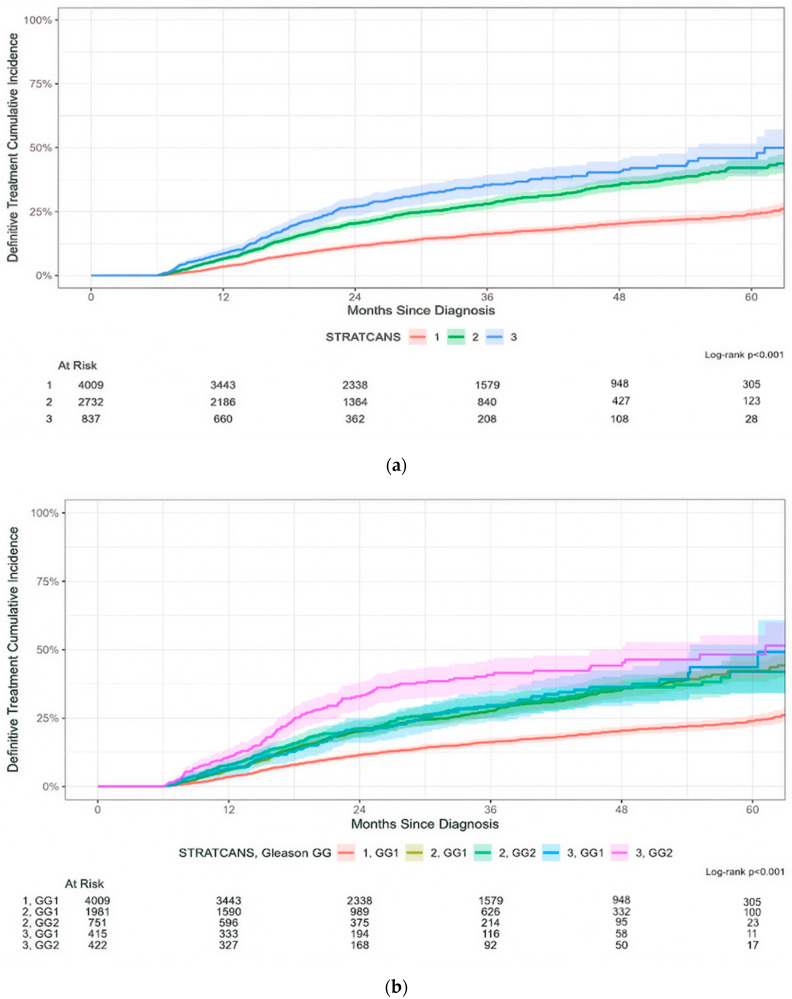
Results: Among 7578 men on AS, 4009, 2732, and 837 patients were in STRATCANS 1, 2, and 3, respectively. The risk of progression to ≥GG3 was 13%, 33%, and 53% for patients in STRATCANS 1, 2, and 3, respectively (p < 0.001). The rate of any biopsy upgrading was approximately 50% at 3 years across all STRATCANS tiers. STRATCANS tiers were also significantly associated with time to definitive treatment, with 16%, 28%, and 35% of men in STRATCANS 1, 2, and 3, respectively, receiving definitive treatment by 36 months. Limitations include confounding inherent to retrospective registry studies, a short 60-month follow-up period, and variability in biopsy method with no centralized pathology and radiology review.
Conclusions: STRATCANS has a stepwise association with the risk of progression to ≥GG3 disease and time to definitive treatment among men on AS in the MUSIC cohort, supporting its use as a risk-based, follow-up approach in men on AS.
期刊介绍:
Cancers (ISSN 2072-6694) is an international, peer-reviewed open access journal on oncology. It publishes reviews, regular research papers and short communications. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


