G Rollo, A Zarfati, G Burini, L Valfre, C Iacusso, I Capolupo, B D Iacobelli, P Bagolan, A Conforti, F Fusaro
{"title":"持续性低输出新生儿乳糜胸:在部分应答者中,我们应该等待多长时间的胸膜切除术?","authors":"G Rollo, A Zarfati, G Burini, L Valfre, C Iacusso, I Capolupo, B D Iacobelli, P Bagolan, A Conforti, F Fusaro","doi":"10.1002/ppul.71311","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The aim of our study was to review our experience regarding the management of neonatal chylothorax, with particular focus on outcomes of partial responders.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of neonatal chylothorax cases between January 2015 and December 2023. First-line management included drainage, fasting, parenteral nutrition, and octreotide. Good responders had a drainage output of <2 ml/kg/day after 1 week; partial responders had 2-10 ml/kg/day, and non-responders had >10 ml/kg/day or >100 ml/day for 5 days with complications. Partial responders continued conservative management, while non-responders received second-line treatment with bedside iodopovidone chemical pleurodesis.</p><p><strong>Results: </strong>Thirty-five newborns (15 females, 20 males) were diagnosed with chylothorax, 11 congenital and 24 acquired (18 CDH, 5 esophageal atresia, 1 caval thrombosis). After first-line treatment, 7 (20%) were good responders, 19 (54%) were partial responders, and 9 (26%) were non-responders. Non-responders received iodopovidone pleurodesis, which resolved the condition in all cases (median time to resolution was 4 days). Complications during hospitalization included 8 cases of sepsis (1 fatal), 5 of atelectasis (4 related to pleurodesis), and 4 venous thromboses. Partial responders had significantly more sepsis (p = 0.029) but less atelectasis (p = 0.025) compared to non-responders, with similar resolution times and hospital stays. After a median follow-up of 3 years, there were no recurrences or thyroid dysfunction in the iodopovidone group.</p><p><strong>Conclusions: </strong>First-line conservative management, although initially appropriate, can lead to serious morbidity if prolonged. Timely second-line treatment for partial responders with low-output chylothorax can minimize morbidity and mortality. Bedside chemical pleurodesis with iodopovidone is a safe and effective second-line treatment for refractory neonatal chylothorax.</p>","PeriodicalId":19932,"journal":{"name":"Pediatric Pulmonology","volume":"60 9","pages":"e71311"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12461794/pdf/","citationCount":"0","resultStr":"{\"title\":\"Persistent Low-Output Neonatal Chylothorax: How Long Are We Justified to Wait for Pleurodesis in Partial Responders?\",\"authors\":\"G Rollo, A Zarfati, G Burini, L Valfre, C Iacusso, I Capolupo, B D Iacobelli, P Bagolan, A Conforti, F Fusaro\",\"doi\":\"10.1002/ppul.71311\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The aim of our study was to review our experience regarding the management of neonatal chylothorax, with particular focus on outcomes of partial responders.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of neonatal chylothorax cases between January 2015 and December 2023. First-line management included drainage, fasting, parenteral nutrition, and octreotide. Good responders had a drainage output of <2 ml/kg/day after 1 week; partial responders had 2-10 ml/kg/day, and non-responders had >10 ml/kg/day or >100 ml/day for 5 days with complications. Partial responders continued conservative management, while non-responders received second-line treatment with bedside iodopovidone chemical pleurodesis.</p><p><strong>Results: </strong>Thirty-five newborns (15 females, 20 males) were diagnosed with chylothorax, 11 congenital and 24 acquired (18 CDH, 5 esophageal atresia, 1 caval thrombosis). After first-line treatment, 7 (20%) were good responders, 19 (54%) were partial responders, and 9 (26%) were non-responders. Non-responders received iodopovidone pleurodesis, which resolved the condition in all cases (median time to resolution was 4 days). Complications during hospitalization included 8 cases of sepsis (1 fatal), 5 of atelectasis (4 related to pleurodesis), and 4 venous thromboses. Partial responders had significantly more sepsis (p = 0.029) but less atelectasis (p = 0.025) compared to non-responders, with similar resolution times and hospital stays. After a median follow-up of 3 years, there were no recurrences or thyroid dysfunction in the iodopovidone group.</p><p><strong>Conclusions: </strong>First-line conservative management, although initially appropriate, can lead to serious morbidity if prolonged. Timely second-line treatment for partial responders with low-output chylothorax can minimize morbidity and mortality. Bedside chemical pleurodesis with iodopovidone is a safe and effective second-line treatment for refractory neonatal chylothorax.</p>\",\"PeriodicalId\":19932,\"journal\":{\"name\":\"Pediatric Pulmonology\",\"volume\":\"60 9\",\"pages\":\"e71311\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12461794/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Pulmonology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ppul.71311\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Pulmonology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ppul.71311","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
Persistent Low-Output Neonatal Chylothorax: How Long Are We Justified to Wait for Pleurodesis in Partial Responders?
Aims: The aim of our study was to review our experience regarding the management of neonatal chylothorax, with particular focus on outcomes of partial responders.
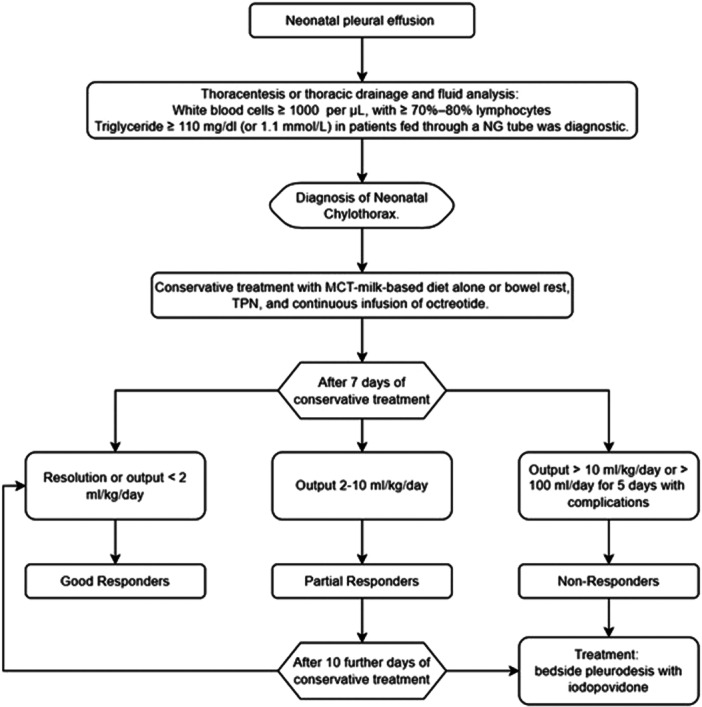
Methods: We conducted a retrospective analysis of neonatal chylothorax cases between January 2015 and December 2023. First-line management included drainage, fasting, parenteral nutrition, and octreotide. Good responders had a drainage output of <2 ml/kg/day after 1 week; partial responders had 2-10 ml/kg/day, and non-responders had >10 ml/kg/day or >100 ml/day for 5 days with complications. Partial responders continued conservative management, while non-responders received second-line treatment with bedside iodopovidone chemical pleurodesis.
Results: Thirty-five newborns (15 females, 20 males) were diagnosed with chylothorax, 11 congenital and 24 acquired (18 CDH, 5 esophageal atresia, 1 caval thrombosis). After first-line treatment, 7 (20%) were good responders, 19 (54%) were partial responders, and 9 (26%) were non-responders. Non-responders received iodopovidone pleurodesis, which resolved the condition in all cases (median time to resolution was 4 days). Complications during hospitalization included 8 cases of sepsis (1 fatal), 5 of atelectasis (4 related to pleurodesis), and 4 venous thromboses. Partial responders had significantly more sepsis (p = 0.029) but less atelectasis (p = 0.025) compared to non-responders, with similar resolution times and hospital stays. After a median follow-up of 3 years, there were no recurrences or thyroid dysfunction in the iodopovidone group.
Conclusions: First-line conservative management, although initially appropriate, can lead to serious morbidity if prolonged. Timely second-line treatment for partial responders with low-output chylothorax can minimize morbidity and mortality. Bedside chemical pleurodesis with iodopovidone is a safe and effective second-line treatment for refractory neonatal chylothorax.
期刊介绍:
Pediatric Pulmonology (PPUL) is the foremost global journal studying the respiratory system in disease and in health as it develops from intrauterine life though adolescence to adulthood. Combining explicit and informative analysis of clinical as well as basic scientific research, PPUL provides a look at the many facets of respiratory system disorders in infants and children, ranging from pathological anatomy, developmental issues, and pathophysiology to infectious disease, asthma, cystic fibrosis, and airborne toxins. Focused attention is given to the reporting of diagnostic and therapeutic methods for neonates, preschool children, and adolescents, the enduring effects of childhood respiratory diseases, and newly described infectious diseases.
PPUL concentrates on subject matters of crucial interest to specialists preparing for the Pediatric Subspecialty Examinations in the United States and other countries. With its attentive coverage and extensive clinical data, this journal is a principle source for pediatricians in practice and in training and a must have for all pediatric pulmonologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


