{"title":"病例报告:高危冠心病患者伴免疫性肾炎糖皮质激素减量后冠脉斑块破裂:机制和临床意义。","authors":"Jianxin Weng, Fushi Piao, Ruihui Lai, Wenwen Chen, Shuai Sun, Tan Xu","doi":"10.3389/fcvm.2025.1625491","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Glucocorticoids (GCs) exhibit metabolic risks that may accelerate atherosclerosis. However, their <i>in vivo</i> effects on atherosclerotic plaques remain poorly understood. This case highlights the perilous interplay between chronic GC use and plaque vulnerability during dose reduction.</p><p><strong>Case summary: </strong>A 51-year-old male with immune nephritis, chronic kidney disease (CKD), and poorly controlled hypertension presented with unstable angina. Coronary angiography revealed multivessel disease [70% stenosis in the proximal left anterior descending artery (LAD) and 90% in the posterior descending artery]. Initial treatment included angioplasty with a drug-coated balloon in the posterior descending artery, dual antiplatelet therapy, statins, and prednisone (10 mg/day). Seven months later, after self-reducing GCs to 5 mg/day, he suffered an acute myocardial infarction due to LAD plaque rupture, confirmed by optical coherence tomography (OCT) showing fibrolipid-rich plaques, deep calcifications, and minimal lumen area (0.67 mm<sup>2</sup>). Emergency stenting was performed to stabilize the patient, with no recurrence at 3-month follow-up.</p><p><strong>Discussion: </strong>This case underscores the mechanistic duality of GCs. Chronic GC therapy suppresses pro-inflammatory cytokines and macrophage activity, stabilizing plaques by reducing oxidized LDL uptake. However, abrupt tapering may trigger rebound vascular inflammation, destabilizing high-risk lesions. OCT imaging proved critical in identifying vulnerable plaque morphology, emphasizing its role in guiding urgent interventions.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1625491"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454324/pdf/","citationCount":"0","resultStr":"{\"title\":\"Case Report: Coronary plaque rupture following glucocorticoid tapering in a high-risk CAD patient with immune nephritis: mechanistic insights and clinical implications.\",\"authors\":\"Jianxin Weng, Fushi Piao, Ruihui Lai, Wenwen Chen, Shuai Sun, Tan Xu\",\"doi\":\"10.3389/fcvm.2025.1625491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Glucocorticoids (GCs) exhibit metabolic risks that may accelerate atherosclerosis. However, their <i>in vivo</i> effects on atherosclerotic plaques remain poorly understood. This case highlights the perilous interplay between chronic GC use and plaque vulnerability during dose reduction.</p><p><strong>Case summary: </strong>A 51-year-old male with immune nephritis, chronic kidney disease (CKD), and poorly controlled hypertension presented with unstable angina. Coronary angiography revealed multivessel disease [70% stenosis in the proximal left anterior descending artery (LAD) and 90% in the posterior descending artery]. Initial treatment included angioplasty with a drug-coated balloon in the posterior descending artery, dual antiplatelet therapy, statins, and prednisone (10 mg/day). Seven months later, after self-reducing GCs to 5 mg/day, he suffered an acute myocardial infarction due to LAD plaque rupture, confirmed by optical coherence tomography (OCT) showing fibrolipid-rich plaques, deep calcifications, and minimal lumen area (0.67 mm<sup>2</sup>). Emergency stenting was performed to stabilize the patient, with no recurrence at 3-month follow-up.</p><p><strong>Discussion: </strong>This case underscores the mechanistic duality of GCs. Chronic GC therapy suppresses pro-inflammatory cytokines and macrophage activity, stabilizing plaques by reducing oxidized LDL uptake. However, abrupt tapering may trigger rebound vascular inflammation, destabilizing high-risk lesions. OCT imaging proved critical in identifying vulnerable plaque morphology, emphasizing its role in guiding urgent interventions.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1625491\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454324/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1625491\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1625491","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Case Report: Coronary plaque rupture following glucocorticoid tapering in a high-risk CAD patient with immune nephritis: mechanistic insights and clinical implications.
Background: Glucocorticoids (GCs) exhibit metabolic risks that may accelerate atherosclerosis. However, their in vivo effects on atherosclerotic plaques remain poorly understood. This case highlights the perilous interplay between chronic GC use and plaque vulnerability during dose reduction.
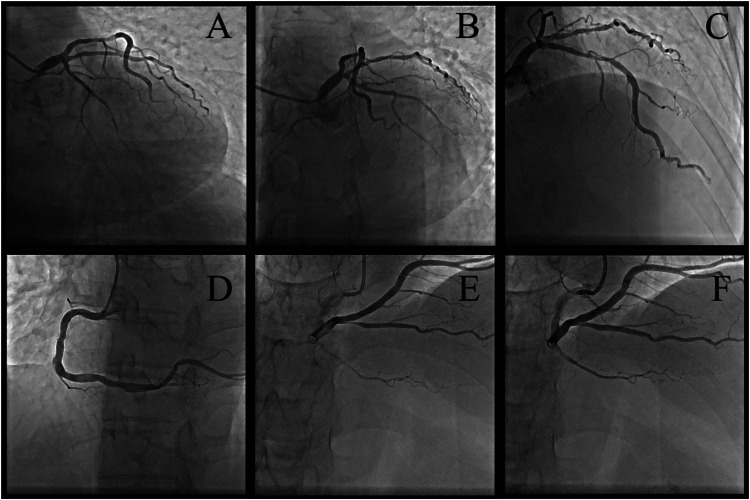
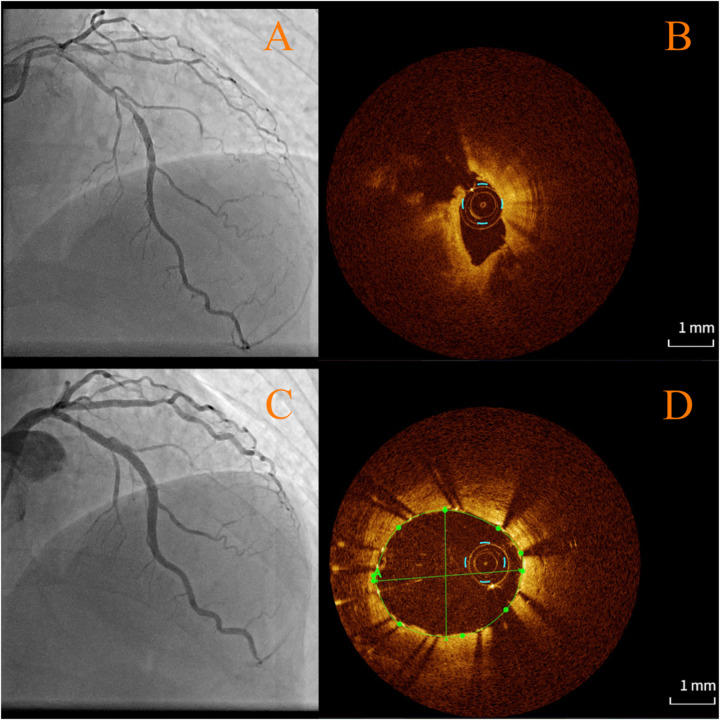
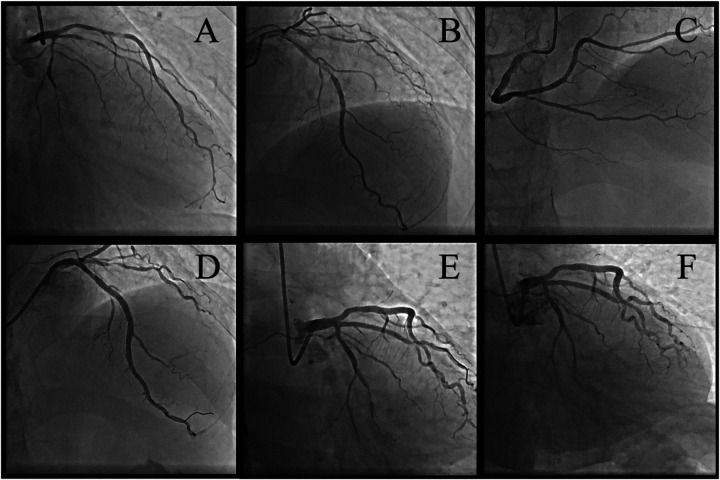
Case summary: A 51-year-old male with immune nephritis, chronic kidney disease (CKD), and poorly controlled hypertension presented with unstable angina. Coronary angiography revealed multivessel disease [70% stenosis in the proximal left anterior descending artery (LAD) and 90% in the posterior descending artery]. Initial treatment included angioplasty with a drug-coated balloon in the posterior descending artery, dual antiplatelet therapy, statins, and prednisone (10 mg/day). Seven months later, after self-reducing GCs to 5 mg/day, he suffered an acute myocardial infarction due to LAD plaque rupture, confirmed by optical coherence tomography (OCT) showing fibrolipid-rich plaques, deep calcifications, and minimal lumen area (0.67 mm2). Emergency stenting was performed to stabilize the patient, with no recurrence at 3-month follow-up.
Discussion: This case underscores the mechanistic duality of GCs. Chronic GC therapy suppresses pro-inflammatory cytokines and macrophage activity, stabilizing plaques by reducing oxidized LDL uptake. However, abrupt tapering may trigger rebound vascular inflammation, destabilizing high-risk lesions. OCT imaging proved critical in identifying vulnerable plaque morphology, emphasizing its role in guiding urgent interventions.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


